Article Text

Statistics from Altmetric.com
- haematology (incl blood transfusion)
- malignant and benign haematology
- gastroenterology
- medical management
Description
A 62-year-old man was referred to casualty with bilateral lower limb swelling and increasing abdominal girth. Prior medical history included type 2 diabetes mellitus and an unprovoked deep vein thrombosis (DVT) 1 year earlier. The patient denied change in bowel habit, gastrointestinal (GI) bleeding, weight loss, anorexia, fever, night sweats or pruritus. Clinical examination showed a distended non-tender abdomen, peripheral oedema and a left pleural effusion.
A CT of the trunk showed focal thickening of the caecum and terminal ileum, extensive peritoneal infiltration and lymphadenopathy, focal thickening of the stomach, mild ascites and left pleural effusion (figure 1). An ultrasound-guided diagnostic ascitic tap revealed a nucleated cell count of 38.1×109/L, (mononuclear cell count 31.25×109). Serum chorioembryonic antigen level was normal. Serum lactate dehydrogenase was 393 U/L (normal range 135–220 U/L). Uric acid was 918 μmol/L (normal range 202.3–416 μmol/L). Liver profile and peripheral full blood count were normal. HIV and hepatitis screen were negative, Epstein-Barr virus PCR was undetectable. Coeliac screen was negative.

CT imaging: (I) marked thickening of the caecum with involvement of the terminal ileum and (II) extensive peritoneal involvement. A, anterior; L, left; P, posterior; R, right.
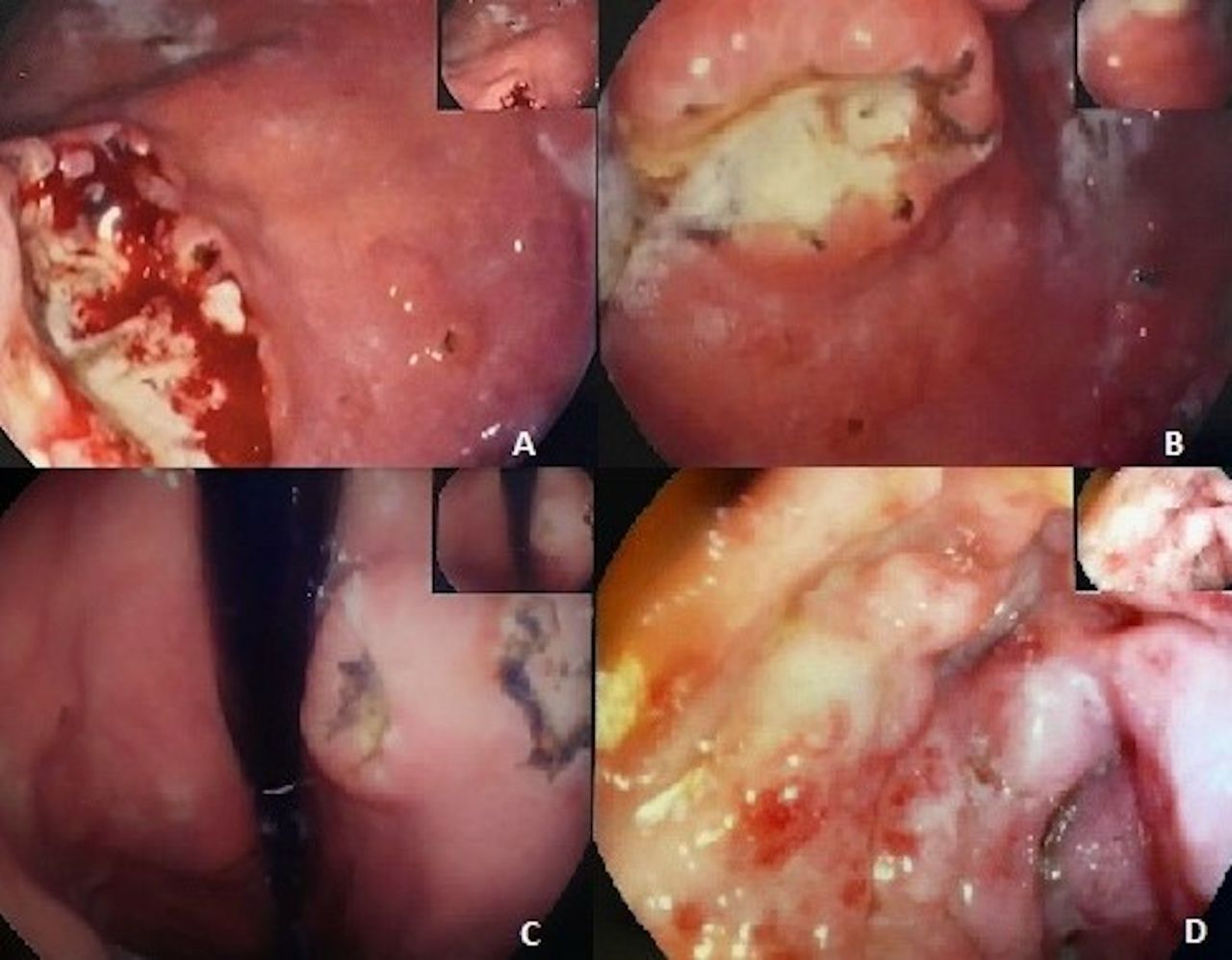
Oesophagogastroscopy (figure 2A–C) showed a 3 cm ulcer in lesser curve of stomach with overhanging edges, together with erosive gastritis. Colonoscopy (figure 2D) revealed thickened folds with oedematous but intact mucosa. Histopathology revealed massive, diffuse infiltration with CD20 and CD10 positive lymphoid cells, consistent with high-grade diffuse large B cell lymphoma (DLBCL). Campylobacter-like organism test was positive for Helicobacter pylori infection. Ascitic fluid cytology and subsequent confirmatory cell block conformed to the diagnosis.

{kind=link}
{kind=link}
Endoscopy findings: (A–C) lymphomatous gastric ulcers and (D) oedematous colonic mucosa.
The patient was referred to the haematology clinic. Positron emission tomography-CT subsequently demonstrated abnormal uptake in the spleen, stomach, bowel mesentery and the left testicle as well as involvement of multiple lymph node groups above and below the diaphragm, in keeping with stage 4A lymphoma (Ann Arbor Classification). R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisolone) regime was prescribed.
The GI tract is the predominant site for extranodal non-Hodgkin lymphomas. DLBCL is the the most common subtype.1 Secondary GI involvement is commoner than primary GI lymphoma, the latter accounting for about 15%–20% of GI lymphomas. The stomach is most commonly involved (75%), followed by small bowel (9%) and ileocaecal region (7%). Furthermore, 6% have more than one GI site involved, and diffuse colonic involvement is seen in 1% of cases.2 Studies have shown that the the most common symptoms include abdominal pain, anorexia and weight loss,3 as well as nausea and vomiting, change in bowel habit, GI bleeding, intussusception and intestinal perforation.4
Dawson et al established criteria for the diagnosis of primary GI lymphoma.5 These include a normal peripheral cell count, predominant tumour involvement in the GI tract, absence of peripheral or mediastinal lymphadenopathy, or liver or spleen involvement.
This case highlights the fact that very advanced disease may present with non-specific and insidious symptoms. Our patient lacked the typical B-symptoms and GI red flag symptoms despite the high disease burden. Interestingly, our patient had had a CT of thorax, abdomen and pelvis (TAP) in the previous year for screening purposes after the unprovoked DVT, with no diagnostic abnormalities noted, highlighting the rapidity of disease progression. In such advanced presentations, it may prove difficult to differentiate between primary and secondary GI lymphomas.
Patient’s perspective
I had never imagined that lymphoma could have been the cause of the swelling I had in both legs. I did not know much about this malignancy so I read about it after I was diagnosed. I never experienced the common symptoms described in the literature and I still cannot believe how rapidly lymphoma can progress. I had a scan of my trunk a year previously after I was diagnosed with deep vein thrombosis and surprisingly it was normal at the time. I have been told that my gastrointestinal tract was one of the main body areas involved—I am surprised that this can happen without any related symptoms.
On a different note, I am grateful for the care provided by my medical team while undergoing investigations and I look forward for a positive response to the chemotherapy that I am having.
Learning points
Lack of red flag symptoms, a normal blood count and other blood investigations do not preclude extensive lymphomatous gastrointestinal involvement and may not parallel disease burden.
A very high peritoneal fluid mononuclear cell count may be the only pointer towards diffuse abdominal lymphoproliferative disorders in the absence of imaging.
Lymphoma can present with very non-specific and insidious symptoms that warrant thorough investigations, if not explained by commoner pathology.
Acknowledgments
The authors would like to thank Professor Emanuel Farrugia who was the patient’s caring consultant.
Footnotes
Contributors MB and SM were both involved with the direct care of the patient, as well as writing up the case report and discussion.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.