Article Text

Statistics from Altmetric.com
Description
A 7-year-old girl presented with complaints of frequent falls for the past 3 years. She achieved unsupported sitting at 8 months, crawling at 9 months, standing at 11 months, walking at 15 months, running at 20 months. At 3 years of age, she could climb up and down stairs, two steps at a time, dress herself completely including buttoning, feed herself, go to toilet, knew own full name, as well as names of family members and played in a group. After that she had frequent falls, initially while running and it progressed to during walking also over a period of the next 1 year. She had difficulty in getting up from a sitting position and used to climb up with the support on her own legs. At 7 years of age, she was able to walk without support but could not run and climbed stairs with the support of railings. She was born to non-consanguineous parents and her family history was unremarkable. There was no history of feeding and respiratory difficulties.
On examination, she had normal anthropometric parameters, normal cognitive and language function, tongue fasciculations, Gower sign and irregular, small amplitude myoclonic movements of hands suggestive of polyminimyoclonus (video 1), mild hypotonia and proximal muscle weakness affecting legs more than arms (proximal and distal muscle power in bilateral upper limbs was −4 and 4 and in bilateral lower limbs it was +3 and 4, respectively), absent muscle stretch reflexes and bilateral flat foot.
Outstretched hand showing irregular, small amplitude myoclonic movements suggestive of polyminimyoclonus.
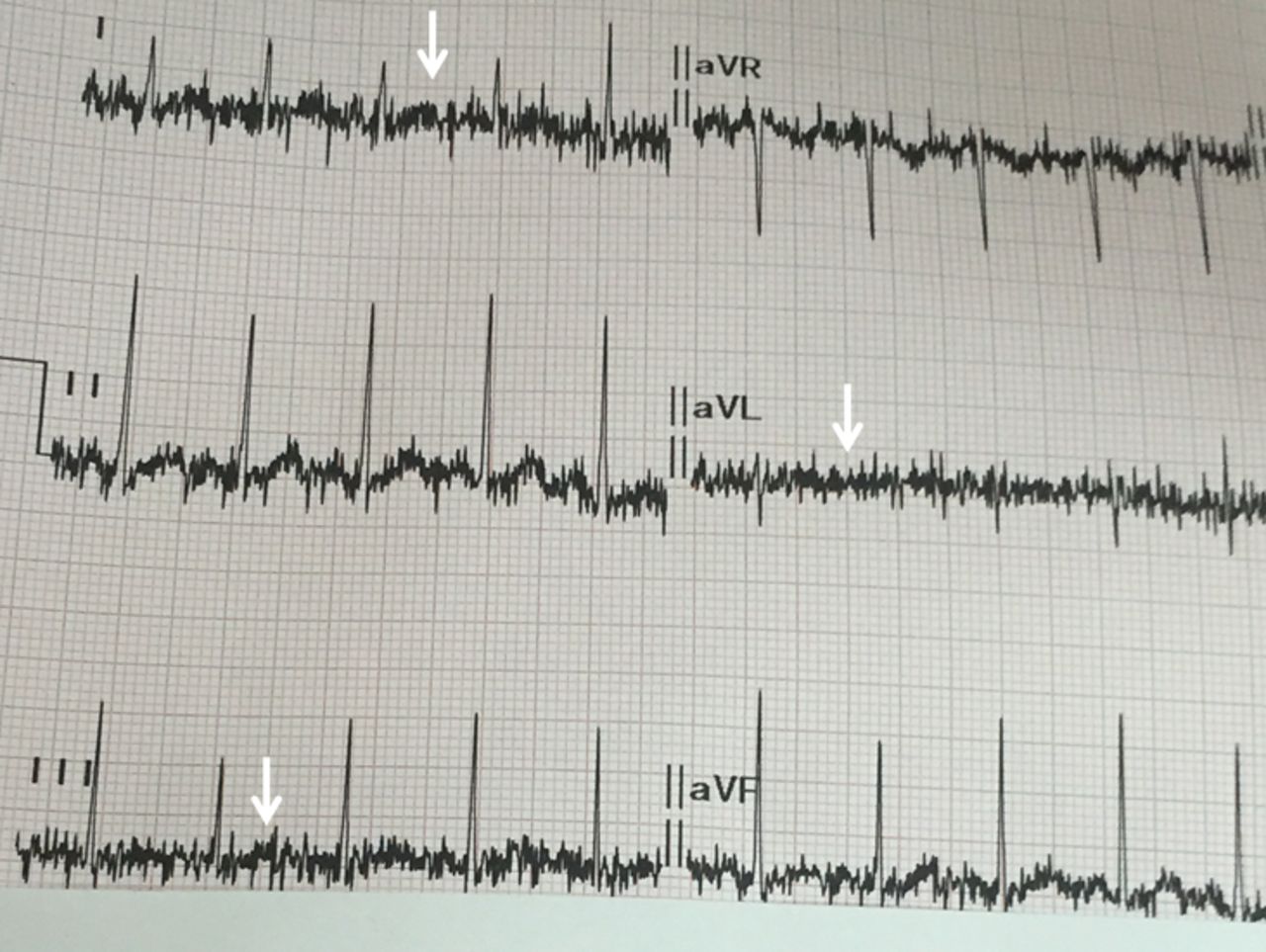
Investigations revealed mildly elevated creatine kinase (322 IU/L), mildly decreased motor unit action potentials on nerve conduction study of right ulnar (2.6 µV) and right tibial nerves (6.4 µV). ECG showed muscle fasciculations above the isoelectric baseline (figure 1). On the basis of clinical history, examination and ECG, a clinical possibility of spinal muscular atrophy type-3B was considered. Genetic test by PCR revealed a homozygous deletion in exon 7 and 8 of SMN1 gene, confirming the diagnosis.

{kind=link}
ECG of the child showing muscle fasciculation as spikes of 40–50 Hz frequency (arrow).
Spinal muscular atrophy (SMA) type-3 also called as Kugelberg–Welander disease is a slowly progressive disorder of anterior horn cells and is caused by mutation in SMN1 gene. Depending on onset of the symptoms, SMA type-3 is further subdivided in to type-3A (onset is between 18 and 36 months) and type-3B (after 3 years).1 Children with SMA type-3 are able to walk without support which differentiates them from other types. They have very slowly progressive proximal muscle weakness and around 50% with type-3B are able to walk independently till the end of the fourth decade. They may have tremors or polyminimyoclonus of hands. Around 50%–60% patients have ECG tremors.2 Chronic re-innervation of the motor neurons produces somatic muscles fasciculation that appears as tremors during ECG.3 Rarely, these patients may have calf hypertrophy and can be confused with Becker’s muscular dystrophy. ECG tremors in the presence of other relevant clinical history and examination can suggest a possibility of spinal muscular atrophy and may be used as a bedside screening tool.
Learning points
Spinal muscular atrophy type-3 also called as Kugelberg–Welander disease is a slowly progressive disorder of anterior horn cells and caused by mutation in SMN1 gene.
Patients with SMA type-3 may have associated tremors and polyminimyoclonus of hands.
Chronic re-innervation of the motor neurons produces somatic muscles fasciculation that appears as tremors during ECG tracing.
ECG tremors in the presence of other relevant clinical history and examination can suggest a possibility of spinal muscular atrophy and may be used as a bedside screening tool.
Footnotes
Contributors IKS and TSK: patient management, literature review and initial draft manuscript preparation. LS: Clinician-in-charge, critical review of manuscript for important intellectual content and final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Parental/guardian consent obtained.