Article Text

Statistics from Altmetric.com
Description
An 18-year-old man presented with complaint of large size lump of 22×18×10 cm in the left axilla for >4 years duration. He also had complaint of restricted movement of left upper limb at shoulder joint. His upper limb was always in the abducted position for last 9 months because of large size of lump in his left axilla (figure 1). The patient had no history of constitutional symptoms including weight loss, loss of appetite, fever, cough or respiratory problem. He had no history of surgery or trauma in axillary or thorax region. On physical examination, in the left axilla, a hard, firm and fixed mass of size 22×18×10 cm was palpable. The lump was non-tender on palpation with irregular margin. There was no impulse on coughing and lump was non-reducible. All laboratory tests were within normal limits. Fine needle aspiration cytology was done two times with non-conclusive result. Patient underwent for surgical exploration under general anaesthesia. Intraoperatively the adherent mass was extended up to subclavian vessels, scapular area and chest wall up to nipple with irregular margin and fibrous consistency (figure 2A,B). The tumour was large in size, gray-white in colour, fibrotic in consistency with irregular margin. The axillary vessels and other accompanying vessels were intact. Total excision of the tumour including intercostal muscles and perichondral tissues were carried out. Pathological examination confirmed the diagnosis of extra-abdominal fibromatosis (EAF). EAF is also known as aggressive fibromatosis (or desmoid tumour).1 EAF constitutes <0.03% of all neoplasm and one-third of all desmoid tumours.2 The most common site for EAF is shoulder and upper limb (33%) followed by lower limb (30%), chest (18%) and head and neck (10%).3 Although MRI is the imaging modality of choice but diagnosis is confirmed histologically with the evidence of abundant collagen mixed with spindle cells, fibroblasts with abundant eosinophilic cytoplasm.3 4 The radical surgical excision at earliest is the best treatment modality and avoid the need of chemotherapy, radiotherapy or hormonal therapy to prevent recurrence.5 6 The axillary fibromatosis is rarely reported in literature and size of 22×18×10 cm is extremely rare.7 On reviewing all the literatures, the largest size of EAF which was 21 cm in size located over chest wall was reported by Agarwal et al.8 The EAF of axilla with largest size were 4×4×3 and 10×8×5 cm3 reported by Pacheco Compaña et al and Duan et al, respectively.5 9 In the series by Kabir et al and Zehani-Kassar et al, the average size of tumour was 6 and 8.75 cm, respectively.10 11 In other two reports by Ali Kaygin et al and Jain et al described the EAF of popliteal region with size of 9 and 8 cm, respectively.12 13 We aim to report this case since to the best of our knowledge this case presents the largest size of EAF in a male patient.

Showing axillary lump of 22×18×10 cm in size.

{kind=link}
{kind=link}
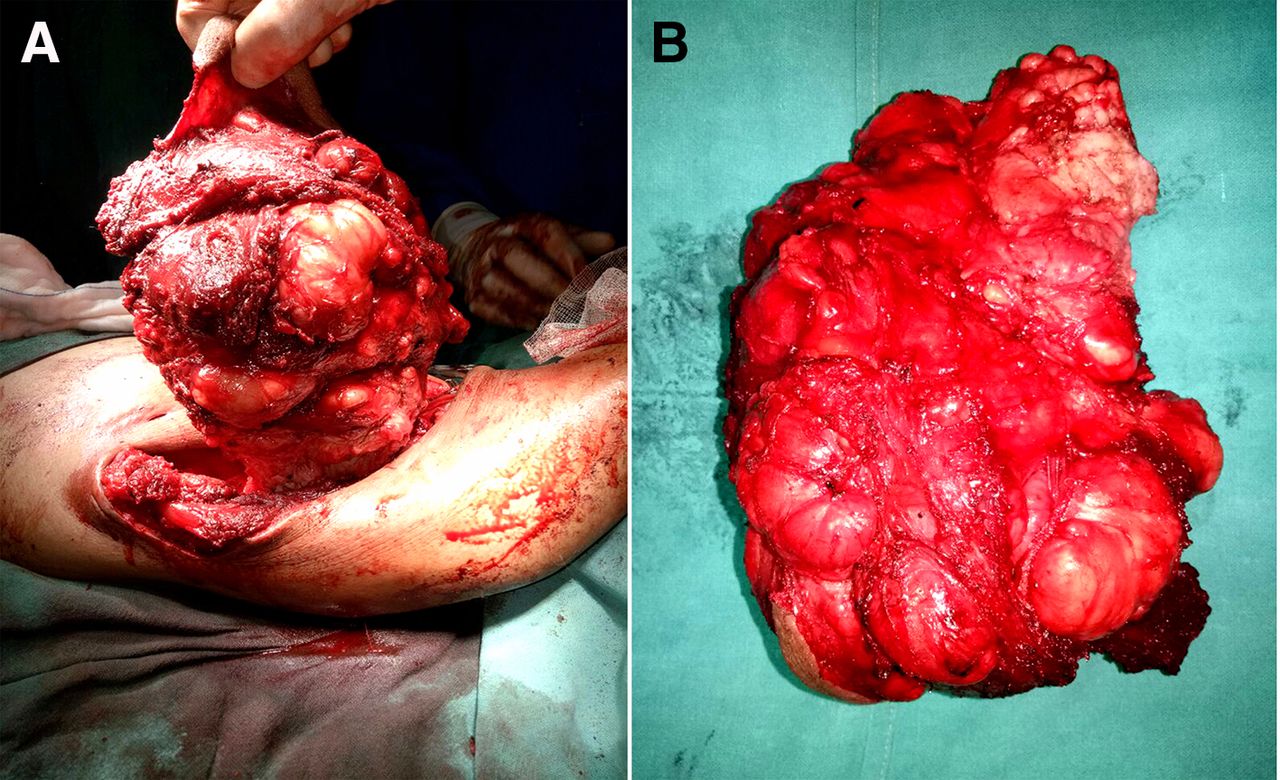
(A) The tumour invading up to the scapula and intercostal muscles. (B) The excised tumour measured 22×18×10 cm in size.
Patient’s perspective
I am very thankful to operating team.
Learning points
Extra-abdominal fibromatosis (EAF) of axilla is extremely rare.
Even the largest size of EAF of axillary region can be excised without damaging to the axillary vessels and in advanced stage reconstruction with vascular graft may be considered.
Chemotherapy is very effective to prevent its postoperative recurrence.
Acknowledgments
The corresponding author would like to thanks to Dr Nishant Sahay, Dr Sanjeev Kumar and Mr Amit Kumar Singh for their help in writing this manuscript.
Footnotes
Contributors AK: operated this case and wrote the manuscript. SK: did CT and MRI. RS: concept of article and HPE. VK: review the whole manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.