Article Text

Statistics from Altmetric.com
Description
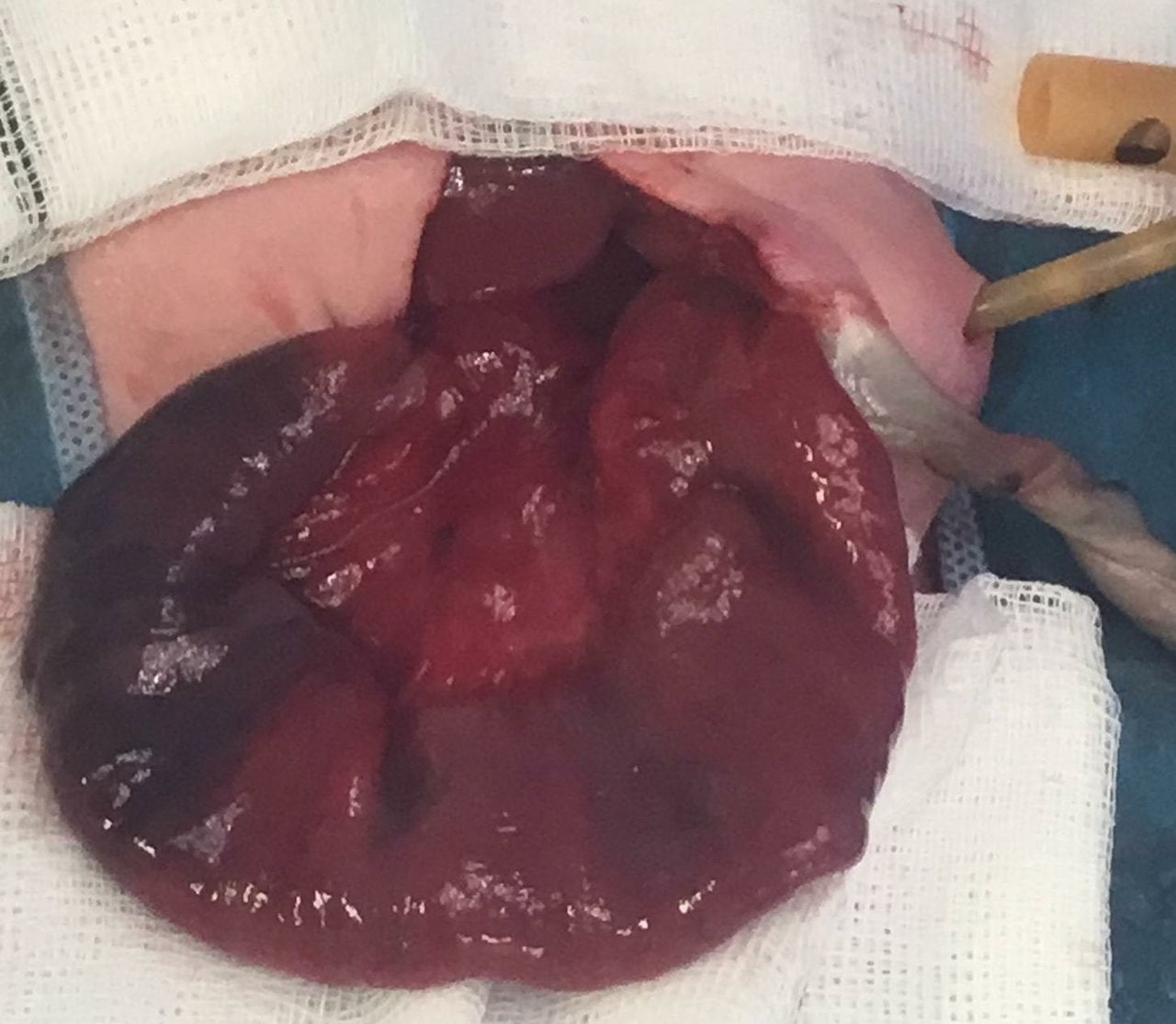
A 32-weeks-gestation, 1.9 kg girl born with emergency caesarean section due to foetal distress. Antenatal scans showed gastroschisis with mild bowel dilatation. At birth, she presented with prolapsed necrotic bowel to the right of the umbilical cord, closed abdominal defect around the small bowel mesentery (figure 1) and with significant haematemesis (initially thought to be ingested maternal blood). After resuscitation, urgent laparotomy revealed complex gastroschisis and vanishing small bowel syndrome. The stomach, duodenum and 20 cm of ischaemic jejunum were twisted 180° intra-abdominally with distal atresia, microcolon and absent ileocaecal valve. The rest of the small intestine has vanished with complete necrosis of the prolapsed intestine through the closing gastroschisis. After untwisting the proximal jejunum and excision of the necrotic bowel (figure 2), a tube jejunostomy was inserted at the bulbous end of the atresia on the left upper quadrant to establish proper drainage of this dilated segment and to avoid re-twisting. Actually, the haematemesis was due to intra-abdominal volvulus with subsequent foetal distress rather than ingested maternal blood. The patient had an uneventful recovery and is currently on long-term home total parenteral nutrition. A bowel lengthening procedure will be considered in the future due to extreme short bowel length <25 cm.

Prolapsed necrotic bowel to the right of the umbilical cord, closed abdominal defect around the small bowel mesentery.

{kind=link}
{kind=link}
Untwisting the proximal jejunum (colour improved gradually) and excision of the necrotic bowel.
Closing gastroschisis is a challenging subset of complex gastroschisis in which the bowel that is eviscerated through abdominal wall defect has been constricted by the fascia resulting in intestinal stricture, atresia, necrosis or resorption.1 2 Based on a recent classification of closing gastroschisis by Perrone et al, this case is defined as Type C (presence of a closing ring with non-viable external bowel with or without an associated atresia). Having <25 cm bowel length, our case is considered having poor prognosis in terms of enteral autonomy.3
Learning points
Gastroschisis is either simple, complex (associated with bowel atresia) or closing gastroschsis with vanishing midgut syndrome.
Haematemesis associated with closing gastroschisis is concerning for bowel ischaemia and surgery should not be delayed.
Ingested maternal blood should be a diagnosis of exclusion opposed to the presumed diagnosis of volvulus.
Footnotes
Contributors Single author work: AAD. The author has operated on this case, wrote the summary and submitted the images. The article was reported and designed by the author.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.