Article Text

Abstract
A 49-year-old man presented to the nearest emergency department profoundly septic with significantly raised inflammatory markers. He had a background of floor of mouth invasive squamous cell carcinoma for which he underwent complex head and neck surgery followed by adjuvant radiotherapy and insertion of a percutaneous gastrostomy tube for feeding. He experienced 3 weeks of retching, cough and malaise. Imaging revealed both an oesophageal perforation and perforated duodenal ulcer, presumed secondary to oesophageal stricturing from his prior surgery and radiotherapy.
- general surgery
- head and neck surgery
Statistics from Altmetric.com
Background
A Boerhaave syndrome is a relatively uncommon form of gastrointestinal perforation, but one which carries a significant mortality risk, particularly if not rapidly diagnosed and treated.1 There have been studies which highlight the difficulty in diagnosing a Boerhaave syndrome and how it can be easily mistaken for peptic ulcer disease.2 In a patient that presents with features of gastrointestinal perforation, with features of sepsis and abdominal pain, especially one that has had prolonged periods of vomiting, it is essential to take a clear history and obtain rapid imaging to ensure there is no delay in diagnosis for an oesophageal perforation.
Case presentation
A 49-year-old man presented to the emergency department with a 24-hour history of severe, generalised abdominal pain with fevers and shortness of breath, preceded by 3 weeks of retching, coughing and general malaise. Five months prior he underwent complex floor of mouth surgery for invasive squamous cell carcinoma (SCC) involving a wide local excision of the SCC, partial mandibular resection and selective neck dissection, and subsequently completed a course of adjuvant radiotherapy. Histopathology of the specimen revealed ulcerated invasive moderateto poorly differentiated squamous cell carcinoma, 25 mm in size with clear margins. There was 0/49 nodal involvement. Due to a severe postradiation oesophagitis he was dependent on percutaneous endoscopic gastrostomy (PEG) feeds for nutrition. It was noted that the patient was not on any proton pump inhibitor therapy at the time of presentation. In addition he had a history of Langerhans cell histiocytosis, took no regular medications prior to his floor of mouth surgery, and had a smoking history of greater than 40 pack years.
On arrival to the emergency department, the patient was febrile at 38.8°C, a heart rate of 110 beats/min with no rhythm abnormalities, a respiratory rate of 24, and was saturating at 97% on 2 L of oxygen delivered via nasal prongs. Clinical assessment revealed a rigid abdomen with generalised peritonitis. Chest examination determined crepitations in the left middle zone, and decreased air entry at the left base with dullness to percussion.
Investigations
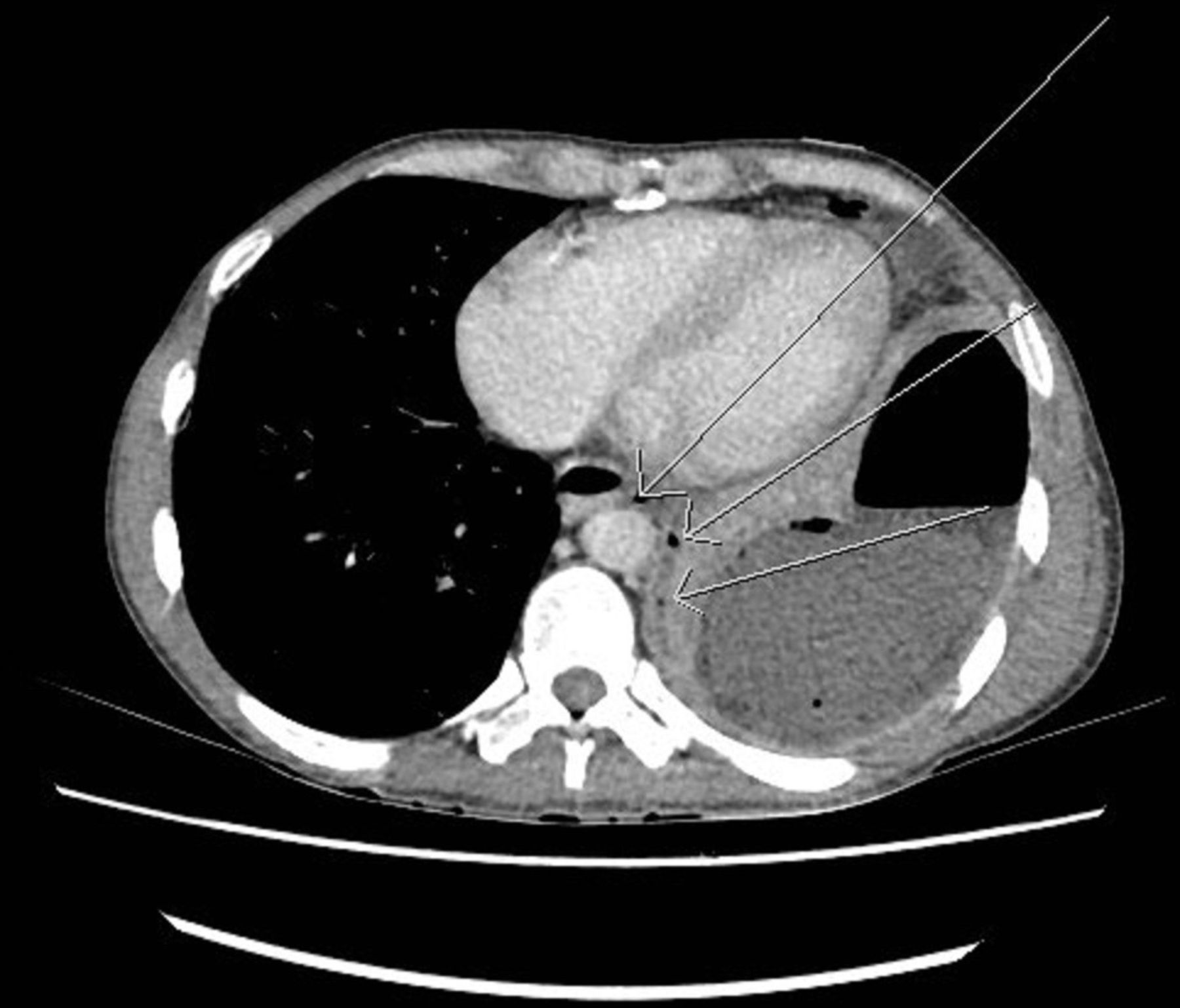
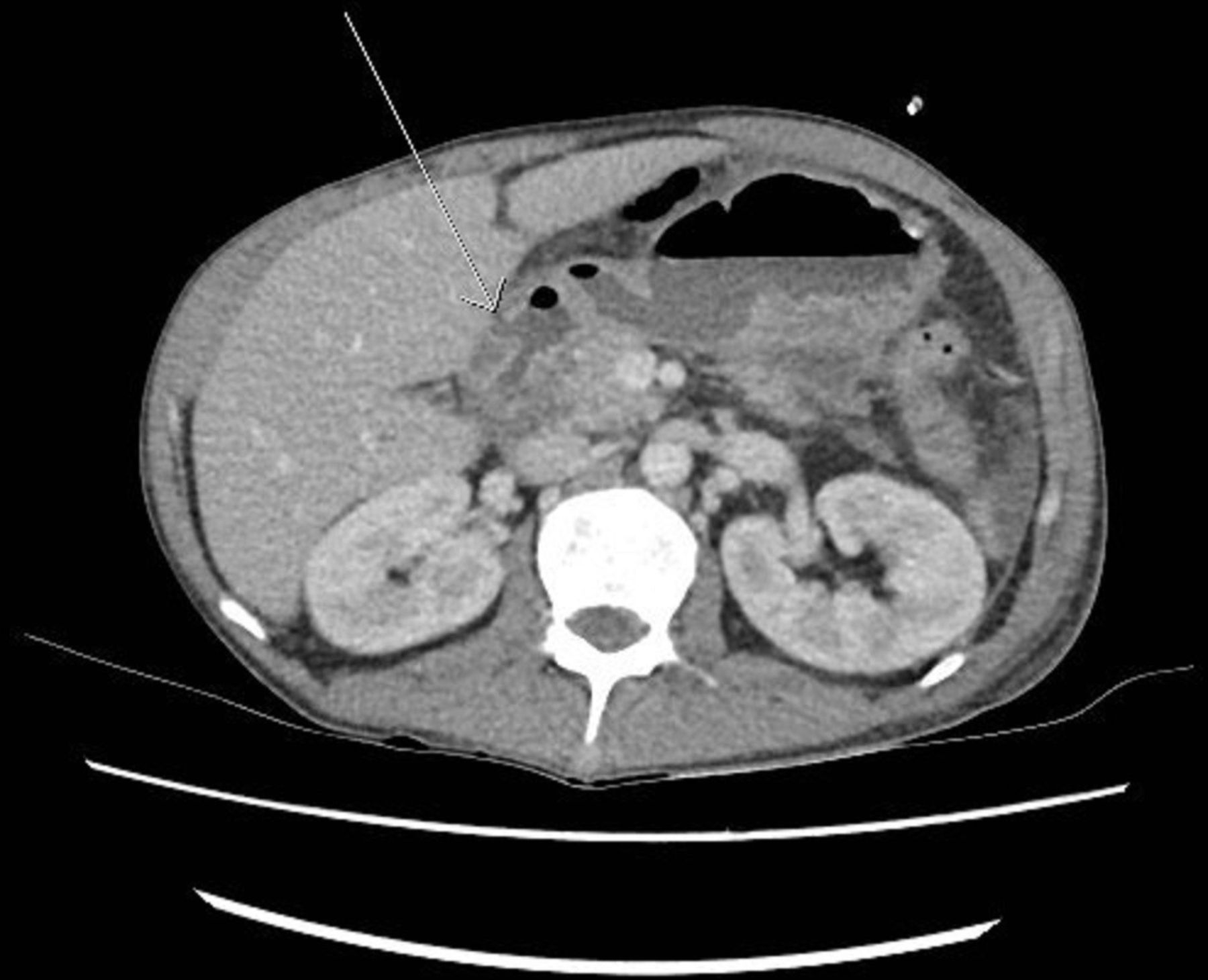
The patient underwent urgent blood tests which returned a haemoglobin of 118, white cell count of 21.42×109/L, platelets of 765×109/L with a C-reactive protein of 280 mg/L. His kidney and liver function were all within normal limits. He underwent a CT scan of his chest and abdomen which demonstrated a left empyema with locules of gas between the left distal oesophagus and the empyema (figure 1) suggestive of Boerhaave syndrome, while there was also noted to be a perforated peptic ulcer at the level of D1 (figure 2).

CT abdomen axial view. Arrows showing gas locules between the distal oesophagus and empyema.

CT abdomen axial view. Arrow showing a perforated peptic ulcer at D1.
Differential diagnosis
As the patient had a presumed intra-abdominal source of sepsis, with severe, generalised abdominal pain, differential diagnoses included a perforated viscus such as an appendix, gallbladder, diverticulum or bowel. However, secondary to the nausea and vomiting, plus the known PEG tube, a perforated gastric or duodenal ulcer was felt more probable. In addition, further abdominal pathology was considered, including bowel ischaemia plus sigmoid or caecal volvulus. While not excluded on clinical assessment, intra-thoracic causes pneumonia and a cardiac event were deemed less likely.
Treatment
The patient was given intravenous piperacillin +tazobactem 4.5 g plus intravenous fluconazole 600 mg, and was administered vigorous fluid resuscitation with Hartmann’s solution. An indwelling catheter was inserted for fluid monitoring, and he was administered high flow oxygen therapy via Hudson mask. He was urgently transferred to the operating theatre and underwent an on-table upper gastrointestinal endoscopy. Since he had radiation induced oesophagitis the oesophagus was not traversable with an adult scope. Instead a paediatric gastroscope (4.8 mm diameter) was used with care through the oedematous proximal oesophagus. Beyond this, the scope identified a linear full thickness defect in the oesophagus at 38–40 cm from the incisors, and severe antral inflammation consistent with peptic ulcer disease. He proceeded to a left posterolateral thoracotomy which revealed copious amounts of pus and presumed refluxed enteral feeds from his PEG feeding regime. Dense fibrous adhesions were encountered in the left chest preventing access to the oesophagus. The left chest abscess cavity was widely drained and the chest closed.
A subsequent midline laparotomy was performed, where a copious amount of enteric contents was encountered within the peritoneal cavity, and a 10 mm defect was identified at the level of D1 and repaired with an omental patch. Since he was unable to swallow due to his recent radiotherapy for his oral SCC and his PEG tube was used only to vent, this largely excluded the perforated oesophagus. A feeding jejunostomy was fashioned 20 cm from the duodeno-jejunal flexure (figure 3).

{kind=link}
{kind=link}
{kind=link}
Illustration by author, Mr Jonathan Foo, of the encountered Intraoperative pathology. A, oedematous oesophagus; B, empyema; C, Boerhaave; D, PEG tube; E, feeding jejunostomy.
Microbiology from the intra-abdominal samples returned streptococcus anginosus, oralis and constellatus plus candida parapsilosis and fusobacterium nucleatum. He was reviewed by the Infectious Disease team and continued on intravenous piperacillin + tazobactem and fluconazole, and later stepped down to a 2-week course of oral amoxycillin + clavulanic acid. He underwent regular chest physiotherapy and speech pathology review throughout the course of his admission.
Outcome and follow-up
The patient made a satisfactory recovery and at the 3-week mark as his oesophagitis settled he was able to swallow small amounts of liquid. A fluoroscopic swallow at 3 weeks demonstrated no leak or stricture of the distal oesophagus. He was discharged at 4 weeks and at 3 months returned to a normal diet. He was followed up in the surgical outpatient clinic at 3 months, and had made an uneventful recovery. A position emission tomography scan was done at 10 months post floor of mouth surgery, which revealed no evidence of residual or recurrent disease, nor any sign of metastatic disease.
Discussion
We hypothesise that this patient developed a stress ulcer in his duodenum leading to delayed gastric emptying. With postradiotherapy strictures in the proximal and middle thoracic oesophagus, and continuous PEG feeds, his resultant vomiting against an obstructed proximal oesophagus led to a barotrauma induced oesophageal perforation. The intrathoracic findings of mature inflammatory changes and dense adhesions are in keeping with a delayed time to presentation, with subsequent perforation of his duodenal ulcer accounting for his acute emergency admission and septic shock.
Boerhaave syndrome is a rare cause of gastrointestinal perforation, but one with a high mortality. A simultaneously diagnosed oesophageal and duodenal perforation within the same patient is a rare circumstance, and highlights the need for thorough examination and investigation.1 Studies have highlighted the difficulty in diagnosing Boerhaave syndrome, and how it can be mistaken for a perforated peptic ulcer.2 Early intervention of an oesophageal perforation significantly improves overall mortality to roughly 6% compared with 40% if the diagnosis is delayed for greater than 24 hours, with an overall mortality of 25%.1 3 However, the literature is sparse on the incidence, aetiology and outcomes of a dual gastrointestinal perforation.
There are limited data regarding the incidence of oesophageal rupture following ear, nose and throat surgery and/or associated radiotherapy, however Tanaka et al,4 identifies three cases of a patient with Boerhaave syndrome following chemoradiotherapy for hypopharyngeal cancer. They hypothesised that chemotherapy induced nausea and vomiting, radiotherapy induced oedema, and stenosis from the tumour burden all contributed to the development of the condition. In addition, a case of dual gastrointestinal perforation was noted in Poland, in a middle-aged man with alcohol dependence syndrome, who presented with severe epigastric pain, dyspnoea, and one episode of profuse vomiting. The patient was noted to have a pneumoperitoneum on a CT abdomen, and fluid in the right pleural cavity. The patient underwent an emergency laparotomy revealing a duodenal perforation, but not until a CT chest 2 days after surgery was arranged due to ongoing patient deterioration was Boerhaave syndrome identified.1
Learning points
In patients with presumed intra-abdominal sepsis, it is essential that differential diagnoses not be limited to the abdominal cavity.
Studies have highlighted the difficulty in diagnosing a Boerhaave syndrome and how it can readily be mistaken for a perforated peptic ulcer.
In patients who are percutaneous endoscopic gastrostomy (PEG) fed for a prolonged period of time, clinicians should be aware of the risk of duodenal inflammation, and the possibility of a resultant duodenal perforation.
Proton pump inhibitor therapy should be considered in all patients with prolonged PEG feeds.
Footnotes
Contributors DH is the primary author. All authors, DH, JF and JR, have contributed to the planning, conduct and reporting of the work described in the article. JF illustrated figure 3.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.