Article Text

Statistics from Altmetric.com
Description
A thriving, previously healthy 3-month-old girl presented with a 4-day history of fever, irritability and poor feeding. On admission, she was tachycardic, had cool peripheries with normal central perfusion, pulse volume and blood pressure. There was no obvious source of infection from clinical examination. Single-bottle blood culture sampling and lumbar puncture were done prior to commencement of ceftriaxone.
Initial blood test revealed an elevated C-reactive protein (CRP) at 214 mg/L and leucocytosis (30.7×109/L), predominantly neutrophils (22.5×109/L), with normal cerebrospinal fluid (CSF) analysis. Blood and CSF cultures were negative. Urine culture grew multiresistant Escherichia coli but it was a contaminated sample with the presence of numerous epithelial cells. Chest X-ray (CXR) was initially reported as normal with prominent thymus.
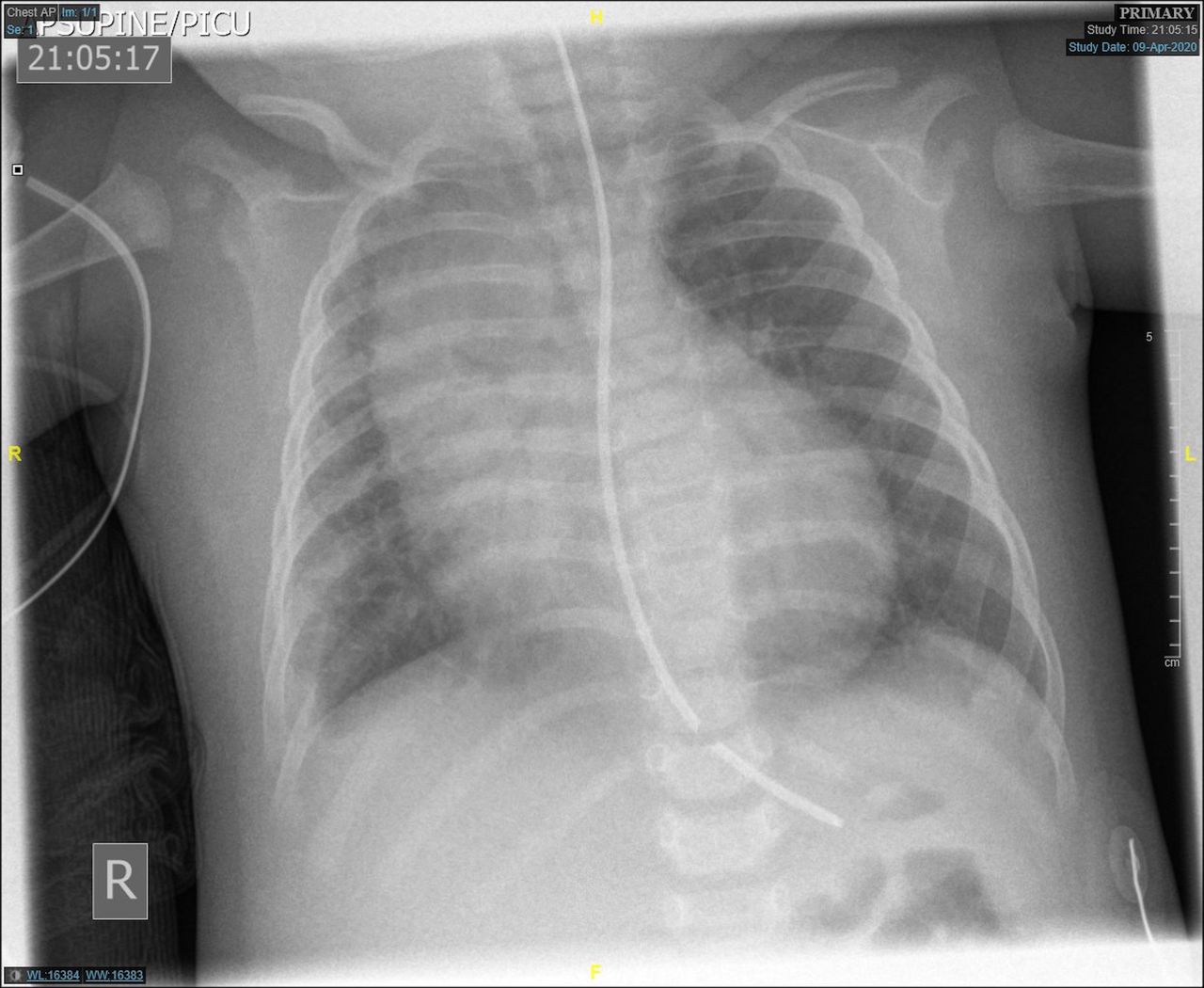
The patient remained febrile (38°C–39.4°C), irritable, persistently tachycardic (160–200 beats/min) and tachypnoeic (57±11 breaths/min) with increasing CRP (highest at 279 mg/L) and leucocytosis (highest white cell count at 43.9×109/L) despite 48 hours of antibiotic treatment. An abdominal ultrasound did not show abnormalities. Besides sinus tachycardia, electrocardiogram was normal. Echocardiography was requested for possible atypical Kawasaki disease and it demonstrated a large echogenic pericardial effusion with fibrous strands, indicative of purulent pericarditis, along with evidence of impending temponade (figure 1). It was thought that the initial CXR actually showed widened mediastinum in addition to prominent thymus. This was confirmed with a second CXR which also revealed globular heart, right chest wall swelling and right pleural effusion (figure 2). The patient subsequently underwent midline sternotomy for surgical drainage. Intraoperative findings revealed large purulent pericarditis and superior mediastinal abscess which extended into the apex of the right lung, the base of the neck along the pretracheal fascia and the right pleural space. The thymus gland was tensed and infiltrated with pus.

Large echogenic pericardial effusion with fibrous strands in echocardiography image. Green and red lines indicate visceral and parietal pericardium, respectively.

{kind=link}
{kind=link}
Second chest X-ray showed widened mediastinum, globular heart, right chest wall swelling and right pleural effusion.
Postoperative computerised tomography (CT) showed a residual rim enhancing abscess in the right superior mediastinum and extensive thrombus in the extracranial right internal jugular vein, indicative of a Lemierre-like syndrome.1 2 CT scan of the head and neck did not demonstrate any infective focus which may have contributed to the diagnosis. Pus culture grew Panton-Valentine leucocidin-producing methicillin-sensitive Staphylococcus aureus.
Intravenous flucloxacillin and clindamycin were given for 4 weeks followed by 2 weeks of oral flucloxacillin with significant clinical and laboratory improvement. Enoxaparin was initiated for a minimum of 6 weeks. Lymphocyte subsets, dihydrorhodamine test, immunoglobulin levels and human immunodeficiency virus (HIV) test did not identify any underlying immunodeficiency.
Purulent pericarditis and mediastinal abscess are very rare3 4 especially in previously healthy children. Infective mediastinitis usually occurs as a result of post-sternotomy complication or due to descending infection from deep neck abscess (eg, peritonsillar, parapharyngeal, retropharyngeal abscesses) and odontogenic infection.4 5 Common aetiologies of bacterial pericarditis in childhood include S. aureus, Mycobacterium tuberculosis (especially in tuberculosis endemic countries), Streptococcus (eg, pneumococcus, group A Streptococcus), Haemophilus, Salmonella, meningococcus and Mycoplasma. Purulent pericarditis is a life-threatening condition with increased risk of constrictive pericarditis.6 Treatment delay has been associated with high mortality due to cardiac tamponade.6 Clinical features of purulent pericarditis include chest pain, tachycardia (out of proportion to the degree of fever), hypotension, pulsus paradoxus tachypnoea and pericardial friction rub.
Learning points
Patients with unexplained clinical signs and symptoms who are not responding to seemingly appropriate treatment should always be carefully reassessed to look for alternative diagnosis, so that any underlying sinister condition is not missed.
In a young infant with clinical and laboratory evidence of serious bacterial infection without other apparent source of infection, widened mediastinum may represent mediastinal abscess and globular heart shape may indicate purulent pericarditis.
Purulent pericarditis must be treated aggressively and promptly because it is a life-threatening condition with high risk of mortality and constrictive pericarditis.
Footnotes
KFN and ASBK are joint first authors.
KFN and ASBK contributed equally.
Contributors KFN and ASBK prepared the manuscript. PCBS and GJS reviewed the article prior to submission. All authors approved the draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.