Article Text

Abstract
Transoral drainage of peritonsillar abscess during the COVID-19 pandemic is a high-risk procedure due to potential aerosolisation of SARS-CoV-2. This case describes conservative management of peritonsillar abscess in a 21-year-old male with COVID-19.
- otolaryngology / ENT
- medical management
- infectious diseases
- global health
- emergency medicine
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Background
Transoral drainage of peritonsillar abscess during the COVID-19 pandemic is a high-risk procedure due to potential aerosolisation of SARS-CoV-2. This case has important implications for healthcare workers when assessing patients with potential peritonsillar abscess and considering routine drainage during the COVID-19 pandemic. We demonstrate that peritonsillar abscess may be managed with high-dose intravenous antibiotics and steroid therapy without undue risk to healthcare workers or compromising patient outcome.
Case presentation
A 21-year-old male presented to a regional hospital with a 5-day history of sore throat, fever, progressive odynophagia and voice change. The patient had been in his usual state of health until 5 days before admission, when sore throat and myalgia developed. One day before admission, the patient developed a fever with associated rigors and chills.
On presentation, the patient denied cough, shortness of breath, chest pain, anosmia or gastrointestinal symptoms. Seven weeks prior to presentation, the patient returned from 6 months of travel in Canada and underwent mandatory pandemic home quarantine for 14 days on return. The patient had no history of medical complaints, no current medications and had been asymptomatic while overseas.
On examination, the patient had a right-sided peritonsillar swelling with surrounding erythema, uvula deviation and trismus, consistent with classic clinical presentation of peritonsillar abscess (quinsy). His temperature was 38.9°C, heart rate 66 beats per minute, blood pressure 117/65 mm Hg, oxygen saturation 98% on room air and respiratory rate 16 breaths per minute. There was no stridor or stertor. The patient had blood drawn for full blood count, urea, electrolytes and creatinine, liver function tests, D-dimer, C reactive protein, procalcitonin and coagulation studies, and a nasopharyngeal swab was performed.
A rapid assay (Cepheid Xpert Xpress SARS-CoV-2 PCR) on the nasopharyngeal swab indicated detection of SARS-CoV-2 RNA. A formal SARS-CoV-2 assay (Roche 6800/800 SARS-CoV-2 PCR assay) confirmed the presence of SARS-CoV-2 RNA. The patient’s white cell count was 14.2×109/L (reference range, 3.5×109/L to 11.0×109/L) with a neutrophilia 11.59×109/L (reference range, 1.7×109/L to 7.0×109/L) and lymphopenia 1.16×109/L (reference range, 1.5×109/L to 4.0×109/L), normal D-dimer 0.41 mg/L (reference range, <0.50 mg/L) and raised C reactive protein 156 mg/L (reference range, <3 mg/L) (table 1). An extended respiratory viral panel was negative for concomitant influenza A, influenza B and respiratory syncytial virus infection.
Clinical laboratory results
The patient was transferred to the nearest tertiary referral centre for admission to a COVID-19 isolation ward. Neither routine aspiration nor incision and drainage of the abscess was undertaken given the risk of SARS-CoV-2 aerosolisation. Conservative management with high-dose intravenous antibiotics (benzylpenicillin and metronidazole) and intravenous steroids (dexamethasone) was commenced.
CT examination with contrast confirmed the diagnosis of peritonsillar abscess illustrating a collection of 22.3×19.5 mm in the axial dimension and 23 mm in the craniocaudal dimension, without extension to the parapharyngeal or retropharyngeal space (figure 1).

Right peritonsillar abscess in an otherwise healthy, immunocompetent 21-year-old male with COVID-19.
Serology for SARS-CoV-2 by immunofluorescence on day of admission (5 days from symptom onset) was negative (IgG <10, IgM <10, IgA <10).
Repeat SARS-CoV-2 PCR assay on nasopharyngeal swab was negative 72 hours after admission (8 days from symptom onset).
The patient improved clinically and following 5 days of intravenous antibiotics (10 days from symptom onset), steroid therapy was weaned and antibiotic therapy was de-escalated to oral amoxicillin and oral metronidazole.
The peritonsillar abscess significantly reduced in size over the period of therapy. Repeat serology for SARS-CoV-2 by immunofluorescence (IgG <10, IgM <10, IgA <10) was negative 5 days after admission (10 days from symptom onset). The patient was discharged 7 days from admission (12 days from symptom onset) on oral antibiotics.
Outcome and follow-up
Repeat SARS-CoV-2 PCR assay on nasopharyngeal swab was negative 2 days after discharge (14 days from symptom onset), and repeat serology for SARS-CoV-2 by immunofluorescence demonstrated seroconversion (IgG 40, IgM 10, IgA <10).
Outpatient review 4 days after discharge (16 days from symptom onset) confirmed complete clinical resolution of the peritonsillar abscess with no trismus and normal oral cavity and oropharyngeal examination (figure 2). The patient indicated he was able to eat and drink normally.

Normal oropharyngeal examination at cessation of antibiotic therapy.
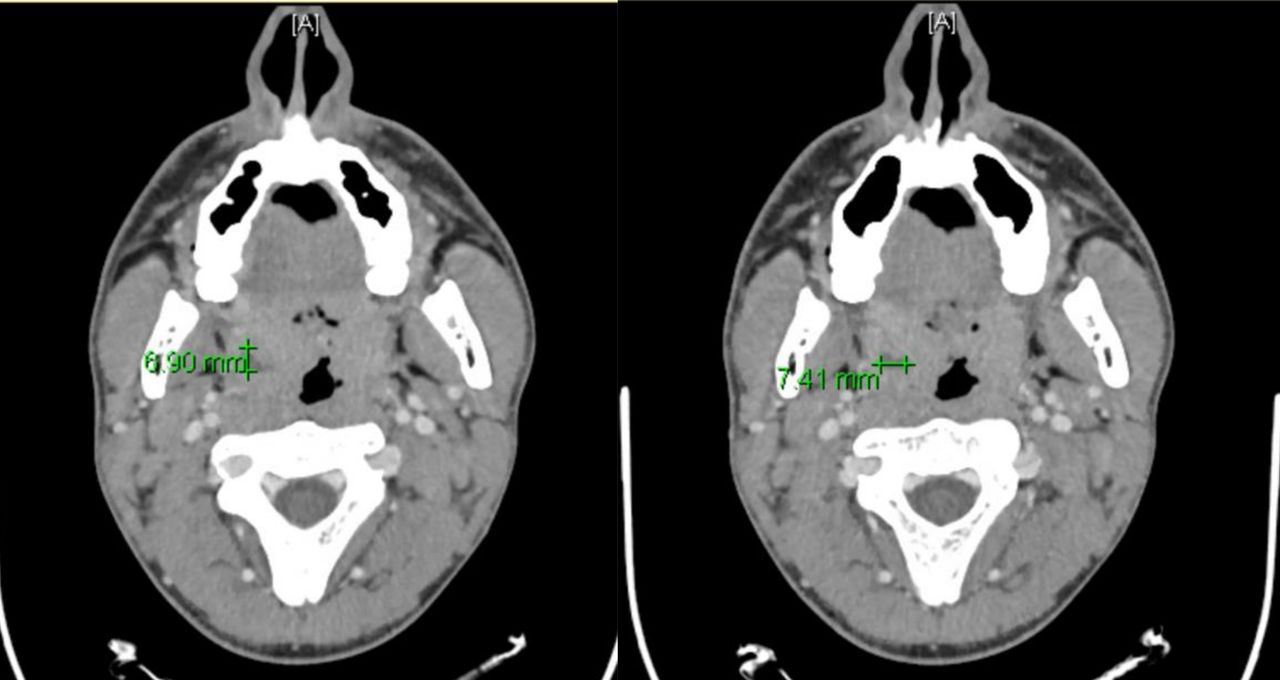
CT examination scheduled 4 days later revealed near total resolution of the peritonsillar abscess (figure 3) and antibiotic therapy was ceased.

{kind=link}
{kind=link}
{kind=link}
CT appearances at completion of antibiotic treatment.
Discussion
This is the first reported case of COVID-19 presenting concomitantly with peritonsillar abscess. The current understanding of the pathophysiology of peritonsillar abscess is the development of a bacterial infection in the peritonsillar space secondary to viral upper respiratory tract infection, acute bacterial tonsillitis or dissemination of bacteria from peritonsillar salivary glands.1 2 This case illustrates that peritonsillar abscess can occur with COVID-19 infection as separate but simultaneous entities.
This case highlights significant risks of routine drainage of peritonsillar abscess3 during the COVID-19 pandemic given it is an aerosol-generating procedure.4 5 Incision and drainage of peritonsillar abscess was first described in the 14th century6 and has remained the mainstay of treatment for peritonsillar abscess, enduring the advent of the antibiotic era. The only available Cochrane systematic review of randomised controlled trials on management of peritonsillar abscess addresses needle aspiration, and incision and drainage, but does not consider conservative management with intravenous antibiotics and steroid therapy alone.3 A recent systematic review of randomised controlled trials on adjunct steroid therapy demonstrated possible shorter recovery time in those treated with needle aspiration or incision and drainage, but not with intravenous antibiotics alone.7
Otolaryngology–Head and Neck Surgery society guidelines for the management of peritonsillar abscess during the COVID-19 pandemic have recommended conservative treatment with medical therapy in cases where airway compromise or systemic sepsis are absent.8 This case demonstrates the only reported implementation of that guideline during the COVID-19 pandemic. Thus, peritonsillar abscess may be managed with high-dose intravenous antibiotics and steroid therapy without undue risk to healthcare workers or compromising patient outcome, as in this case. Limitations of such an approach include prolonged hospital stay (7 days in this case) as opposed to outpatient management.9
This case has important implications for healthcare workers when assessing a patient with potential peritonsillar abscess during the COVID-19 pandemic. At the time of presentation, there had been no new reported local cases of COVID-19 for 5 weeks (despite extensive testing implemented by state government). The total number of new COVID-19 cases in Australia in the 24 hours prior to diagnosis was 12 with a large proportion of active cases identified in returned travellers in mandatory hotel quarantine, indicative of very low community transmission rate.10
This case should remind physicians to maintain a high degree of suspicion in areas of low prevalence of COVID-19, especially when assessing patients with symptoms of upper respiratory tract infection and presentations such as peritonsillar abscess.
Learning points
COVID-19 and peritonsillar infection may present simultaneously and healthcare workers need to be aware of such potential coexistence.
Peritonsillar abscess may be managed with high-dose intravenous antibiotics and steroid therapy without undue risk to healthcare workers or compromising patient outcome.
Maintain a high degree of suspicion in areas of low prevalence of COVID-19, especially when assessing patients with symptoms of upper respiratory tract infection and presentations such as peritonsillar abscess.
Footnotes
Contributors AWS: clinical care of patient, photo acquisition, manuscript writing and editing, approval of final manuscript. NG: Consultant Infectious Diseases physician directing care of patient, manuscript writing and editing, approval of final manuscript. MEL: clinical care of patient, manuscript writing and editing, approval of final manuscript. SGM: Consultant Otolaryngologist Head and Neck Surgeon directing care of patient, manuscript writing and editing, approval of final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.