Article Text

Statistics from Altmetric.com
Description
A 69-year-old man presented to the emergency department with a 2-day history of worsening right iliac fossa pain. He denied any associated nausea, fevers, change in bowel habit, urinary symptoms or recent weight loss. His previous medical history was of hypertension only.
On examination, his abdomen was soft with tenderness in the lower abdomen, but without guarding or percussion tenderness. The initial differential diagnosis at this point included appendicitis or appendagitis. Blood tests on admission were only mildly deranged, with a white cell count of 10.2×109/L and C reactive protein of 87 mg/L, while the remainder were within normal range . Due to the persistence of the pain and clinical equipoise, he subsequently underwent a CT scan of the abdomen and pelvis. The scan was initially reported as showing no evidence of acute intra-abdominal pathology.
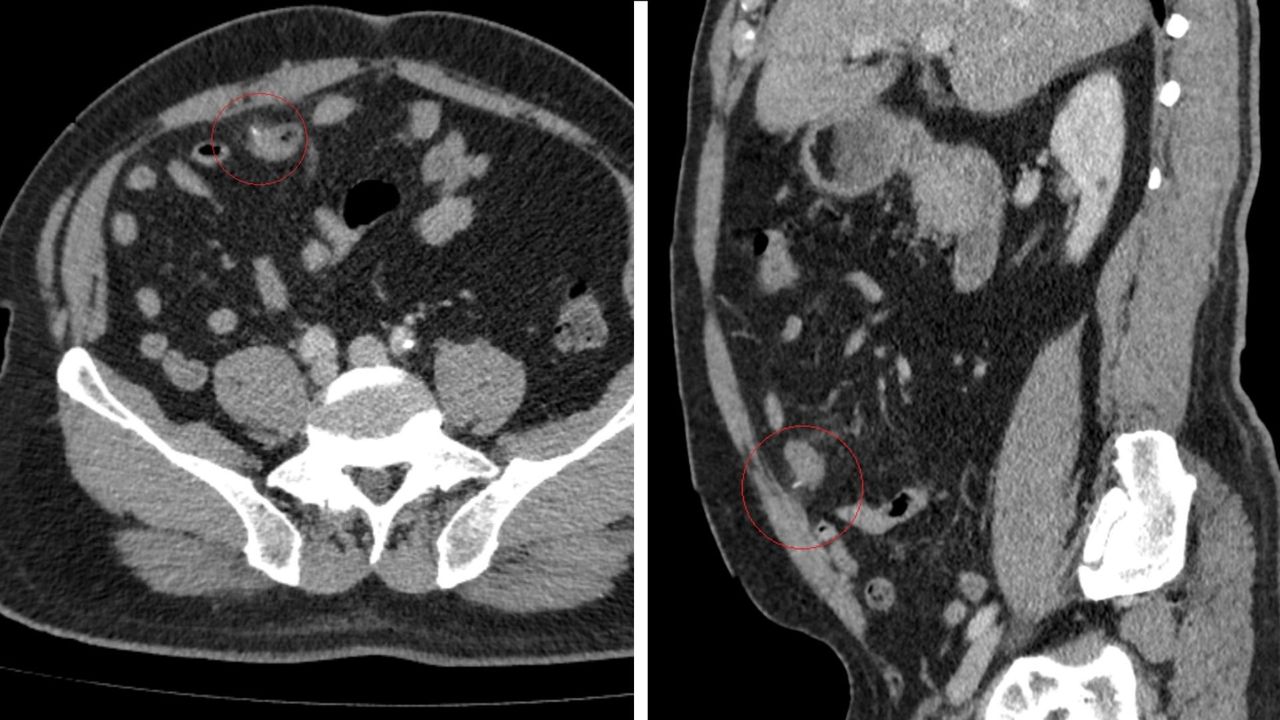
The patient remained in considerable pain, therefore the scan was rediscussed with a senior radiology consultant; a high attenuation linear foreign body was noted in the mid small bowel, extending beyond the lumen and into the omental fat and associated focal stranding of the small bowel mesentery (figure 1). These were noted to be consistent with a fishbone perforation of the small bowel; on further questioning, the patient did recall eating a bony fish 4 days prior to admission.

A transverse (left) and sagittal (right) slice of a CT scan of this patient’s abdomen, demonstrating radiologically the foreign body perforation.
As a result, the patient underwent a diagnostic laparoscopy, which did indeed demonstrate a foreign body, most likely a fishbone, perforating the distal small bowel (figure 2), being sealed off by the omentum. There was no obvious collection or contamination of the abdominal cavity, therefore the fishbone was removed and the decision was made to repair the injury with a single layer of interrupted PDS (polydioxanone) 3.0 sutures overlapping the defect. The postoperative recovery was unremarkable and the patient was discharged 3 days postoperatively.

{kind=link}
{kind=link}
Laparoscopic images demonstrating the perforating fishbone (left) and primary suture repair (right).
Although ingested dietary foreign bodies cause perforation in <1% of cases,1 they often present a diagnostic challenge due to their subtle and variable radiological appearance. Moreover, patients are often unaware that they have ingested anything to cause such a pathology.2 This case highlights the importance of a senior radiological opinion when the clinical picture may not be consistent with the radiological findings. Small bowel perforations by fishbones without any significant bowel injury or contamination can be successfully managed with a primary laparoscopic approach, without requiring any bowel resection.
Learning points
Small bowel perforations by fishbones without any significant bowel injury or contamination can be successfully managed with a primary laparoscopic approach.
Fishbone bowel perforation is often a difficult radiological diagnosis, therefore, additional radiological opinion should be sought if clinical suspicion remains high.
Clinicians should maintain a high index of suspicion with unexplained persistent abdominal pain, when there is genuine equipoise regarding a diagnosis.
Ethics statements
Patient consent for publication
Footnotes
Contributors MZ: obtained patient consent, wrote first draft, created figures. MB: assistant surgeon during the operation, edited the draft, obtained CT images. GK: primary surgeon during the operation, edited the draft. PG: responsible consultant for the patient, edited the draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.