Article Text

Abstract
Herniation of the tympanic membrane is a rare benign malformation of the tympanic membrane into the external auditory canal. It may be asymptomatic or associated with symptoms such as aural fullness, tinnitus, otalgia or hearing loss. We present a case of a symptomatic herniation of the tympanic membrane and its surgical therapy with hernia excision and tympanoplasty. An internal review board exemption was obtained.
- ear
- nose and throat/otolaryngology
- otitis
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Although bulging of the tympanic membrane is commonly encountered, a ballooning herniation occupying the external auditory canal is extremely rare. The development of these lesions is thought to require a pre-existing defect of the tympanic membrane and recurrent positive pressure inside the middle ear. Habitual Valsalva manoeuvres, the so-called ‘autoinflation’, can transiently relieve symptoms in these patients but are also part of the pathomechanism in the first place. Severe cases are recommended to be treated surgically, while in mild cases observation may be a reasonable approach.
Case presentation
A 30-year-old otherwise healthy Swiss Military Officer presented to his local otolaryngologist for an episode of otitis media with effusion on the right side. The water sports enthusiast priorly had a 10 -year history of recurrent episodes of acute otitis media on the affected side. These were often accompanied with perforation of the tympanic membrane and otorrhea but showed spontaneous remission each time. The patient had been treated with antibiotics three times during the last 12 months and reported about hearing loss and a nonpulsatile permanent tinnitus (murmur) on the right side at presentation. He claimed intermittent slight otalgia but denied otorrhea or vertigo. Habitual Valsalva manoeuvres helped to improve the hearing ability.
Once again, the effusion resolved spontaneously after conservative treatment, but on the next presentation, 2 months later, the local otolaryngologist noticed a mass of unclear origin within the proximal external auditory canal. The formation persisted during two subsequent examinations in the following month. A needle aspiration revealed no substance, and the patient was referred to our clinic for further evaluation.
Investigations
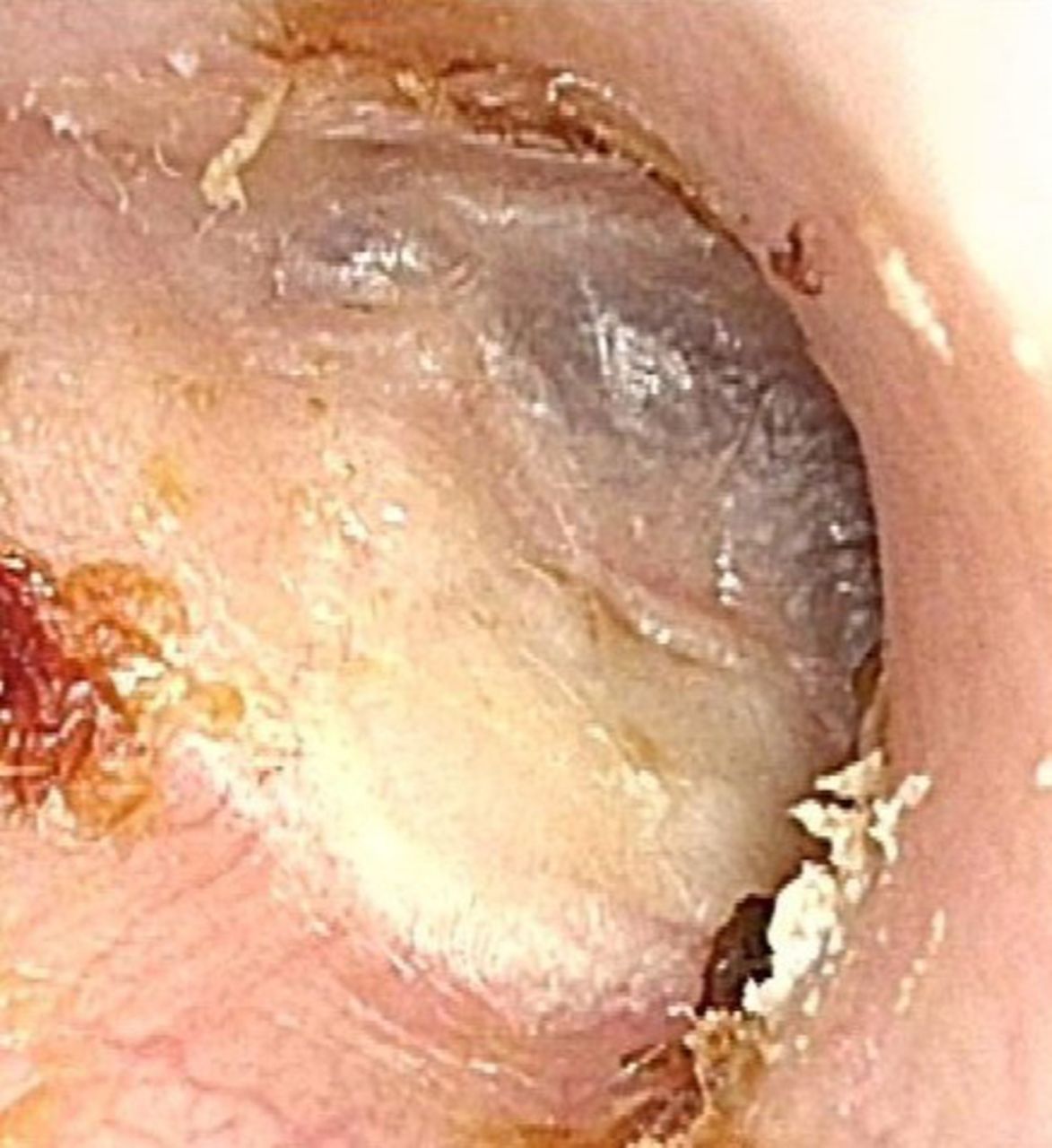
On physical examination, ear microscopy of the proximal auditory canal presented a skin coloured, nonpulsating, round smooth bullous mass with sporadic telangiectasia, which was soft on palpation with blunt instruments. The estimated diameter was 7 mm occupying almost the entire proximal auditory canal, which did not allow to distinguish, whether the formation originated from the tympanic membrane or was situated laterally in the ear canal (figure 1). Valsalva manoeuvre was negative and without sound. Weber’s test lateralised to the affected ear and Rinne’s test was bilaterally positive. The rest of the patient’s head and neck examination was unremarkable.

Findings on ear microscopy (right side).
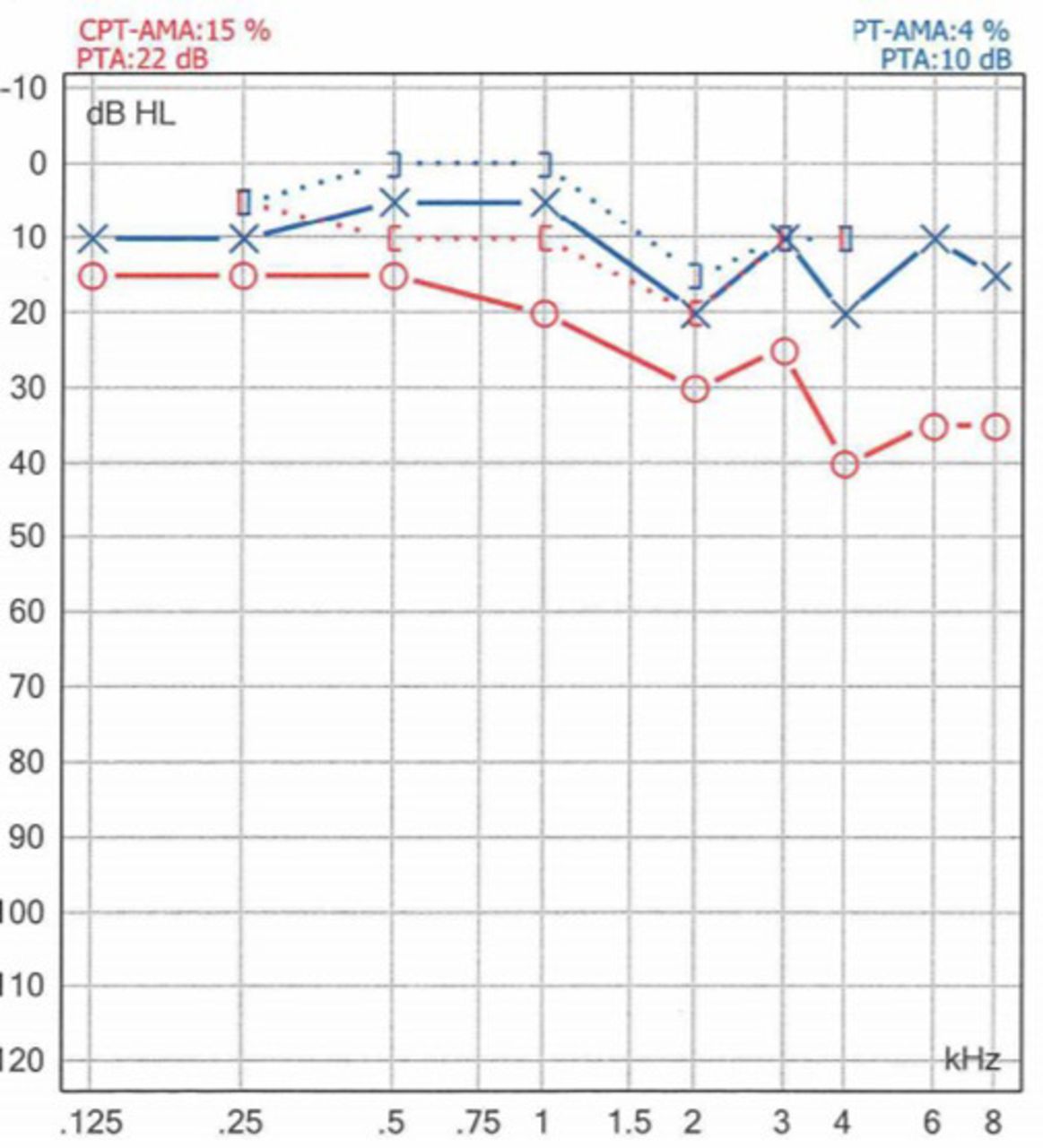
The audiogram demonstrated a symmetric sensorineural hearing function and a moderate conductive hearing loss on the right side with a high-frequency air-bone gap of 10–30 dB HL. Overall hearing loss was 15% on the right side according to the Council on Physical Therapy of the American Medical Association (CPT-AMA) and 4% on the left side (figure 2).

Audiogram. CPT-AMA: Council on Physical Therapy of the American Medical Association.
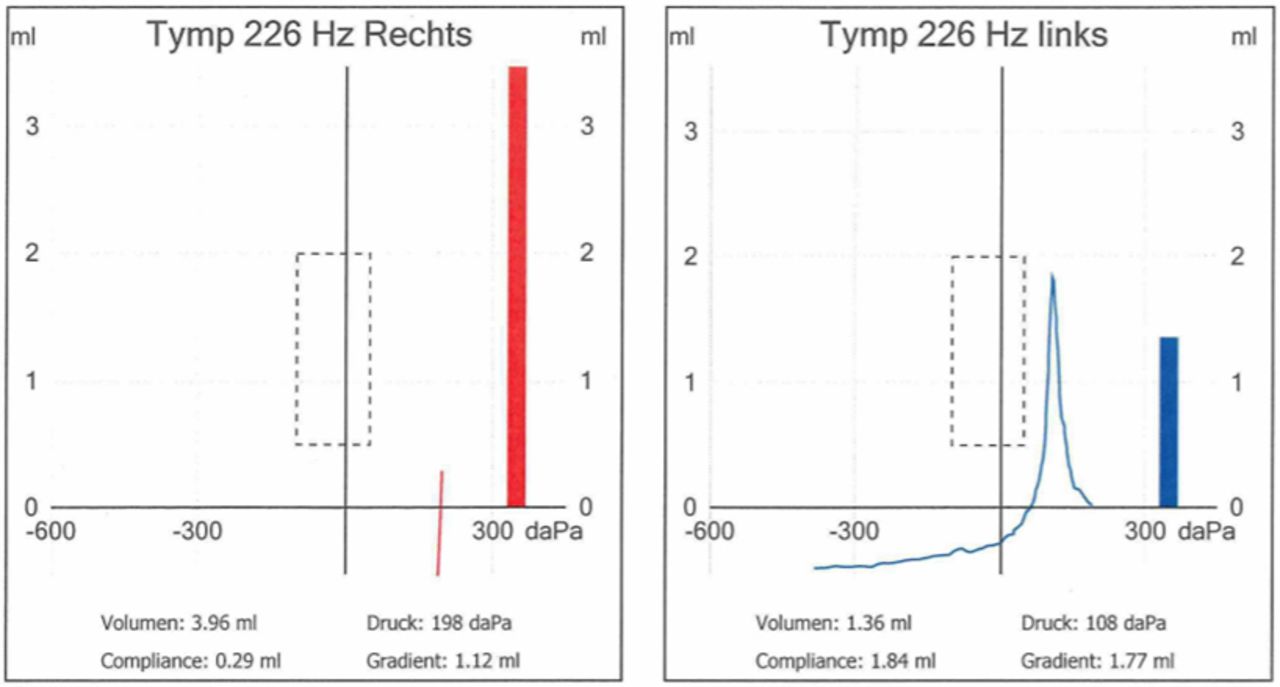
Tympanometry of the right side demonstrated no veritable curve and a high volume of 3,5 mL consistent with a perforation of the tympanic membrane and normal findings on the opposite side (figure 3). The results of tubomanometry showed normal results (30–40 mbar) on both sides.

Tympanometry.
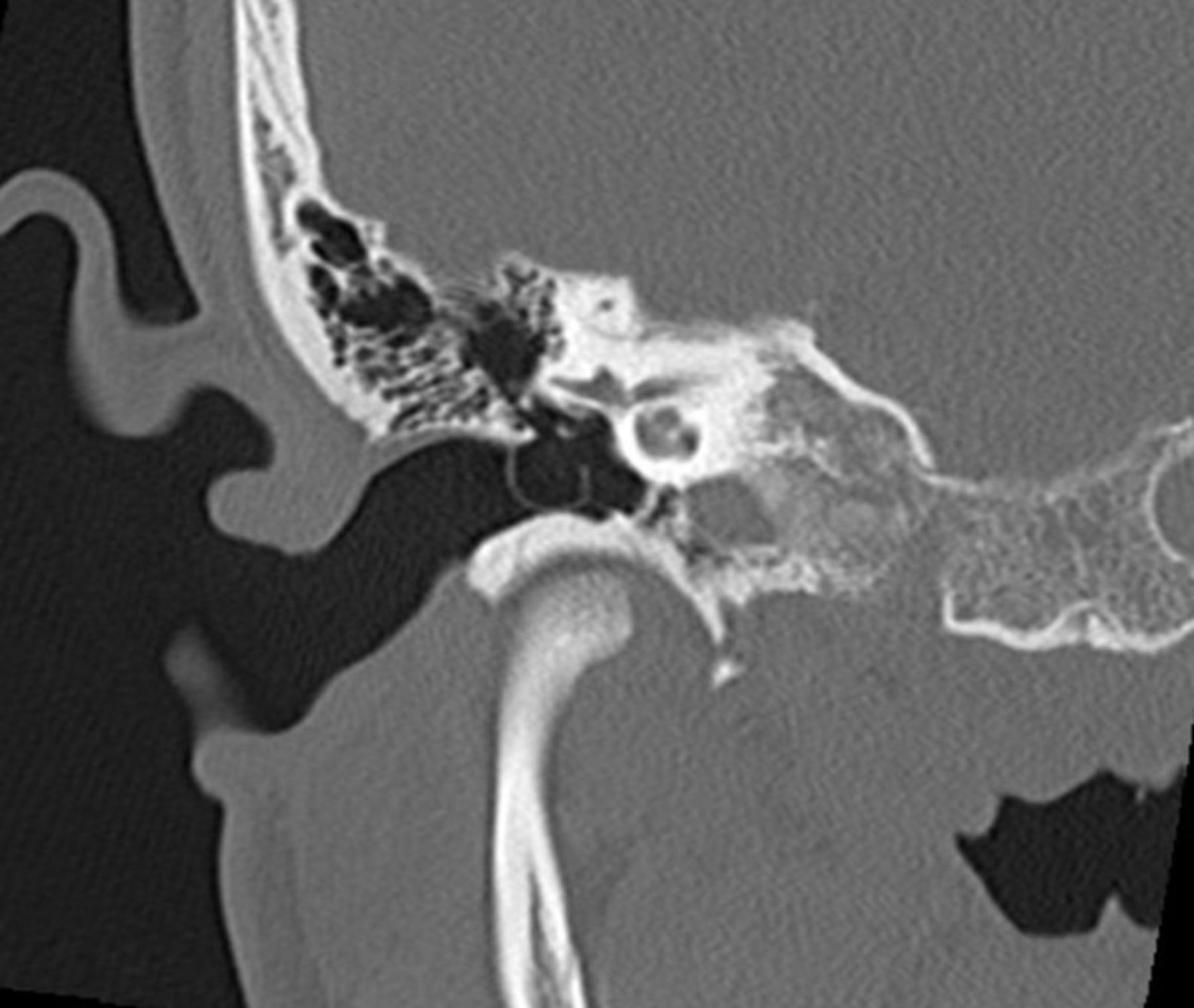
CT scans of the petrous bone were ordered to further evaluation and to exclude destructive lesions of the middle ear. Radiologic imaging demonstrated an extensive lateral herniation of the tympanic membrane of 7 mm in diameter and an otherwise air-filled tympanum without signs of pathologic soft tissue or osseous alterations (figures 4 and 5).

Petrous bone CT scan, axial view.

Petrous bone CT scan, coronal view.
Differential diagnosis
A bullous mass as presented in figure 1 can generally derive from the external ear canal, the tympanic membrane or neighbouring structures such as bones, nerves or in rare cases even the meninges or parotid gland. The overall appearance of the mass in our case with its round, smooth and compressible surface is suggestive for a benign air-filled or liquid-filled cyst, which helps to differentiate from many other possible pathologies.
Primary tumours deriving from the tympanic membrane are extremely rare, but case reports are published about a noncholesteatomous cyst1 as well as capillary haemangioma,2 fibroma,3 schwannoma4 and paraganglioma.5 Benign formations in the external auditory canal include osteomas, dermatofibromas, cholesteatomas6 and ceruminous adenomas.7
A case of an isolated squamous cell carcinoma of the tympanic membrane was published in 2002, but like osteomas, exostosis of the ear canal and advanced stage carcinomas of the parotid gland, these are expected to be more solid on palpation. Taking the incidence as well as the clinical appearance of our case into account, we consider sebaceous cysts of the skin and cholesteatomas of the middle ear or external auditory canal as relevant differential diagnoses.
Petrous bone CT imaging is guiding to evaluate the extent, infiltrative pattern, bone destruction and preoperative anatomy. It helped to confirm our diagnosis by demonstrating an air-filled herniation of the tympanic membrane, which excludes all the above-mentioned pathologies.
To emphasise the importance of preoperative imaging in indefinite lesions, we would like to mention a case of meningioma, which led to bulging of the tympanic membrane and was diagnosed by paracentesis with biopsy.8
Treatment
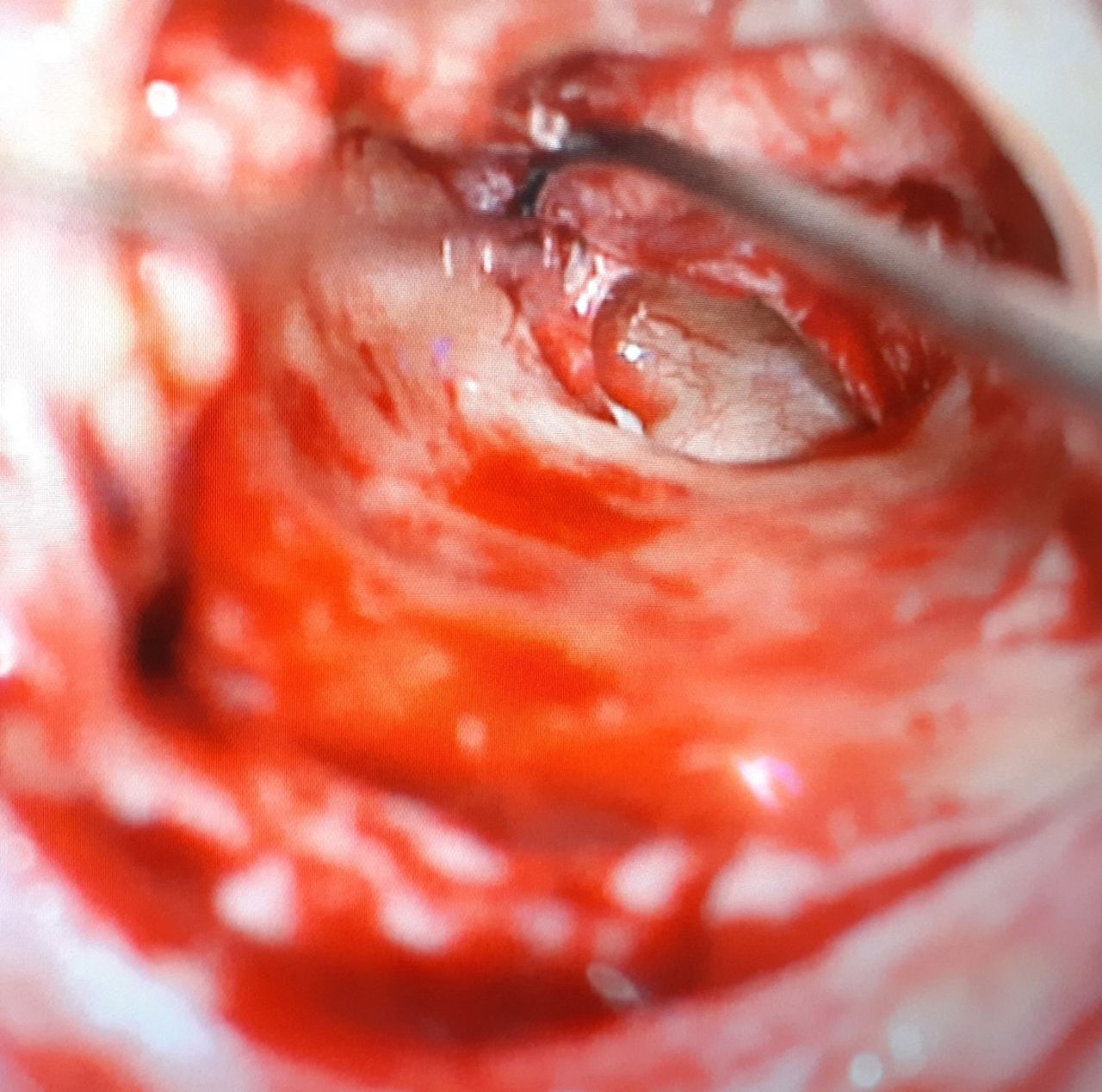
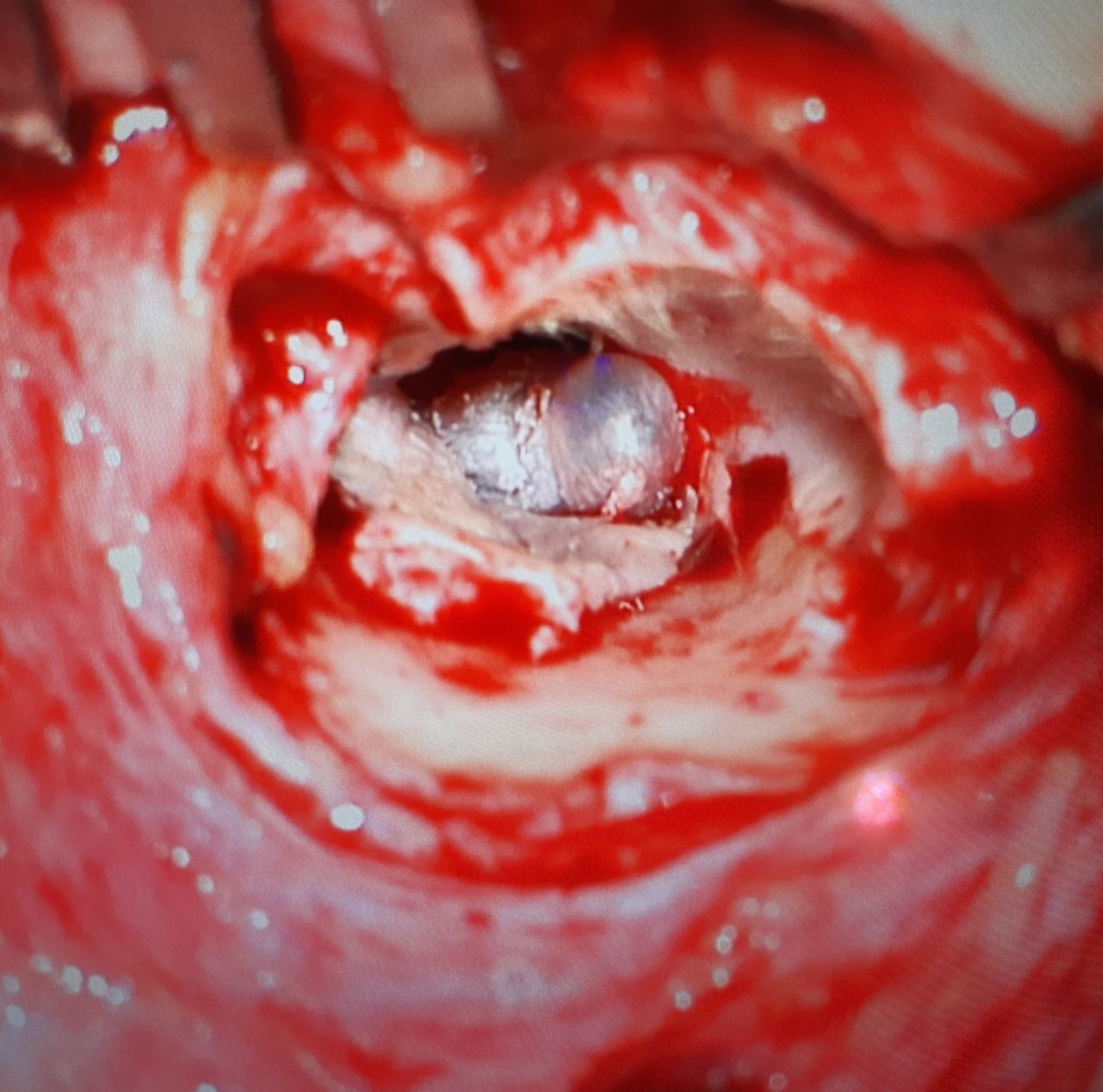
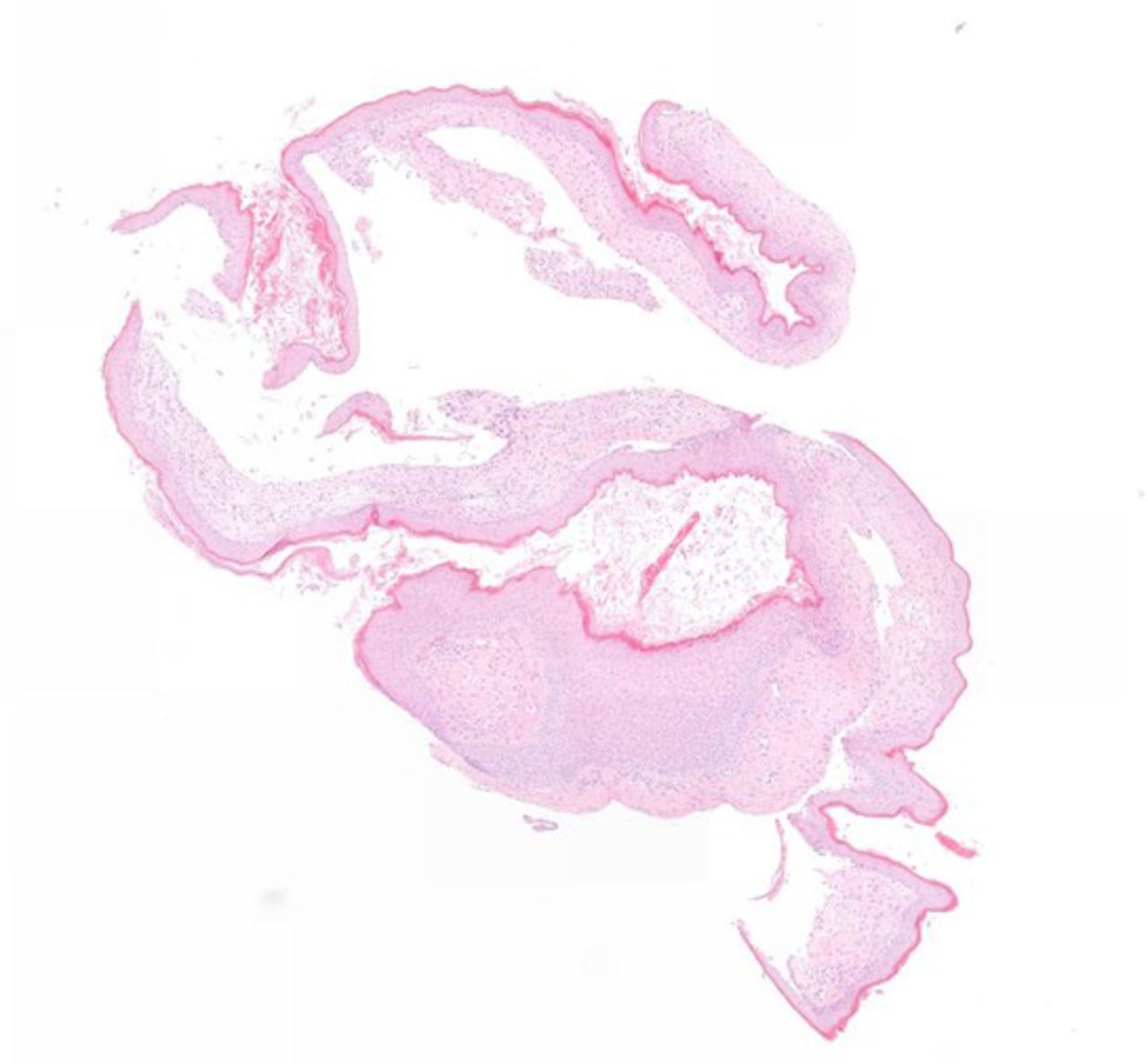
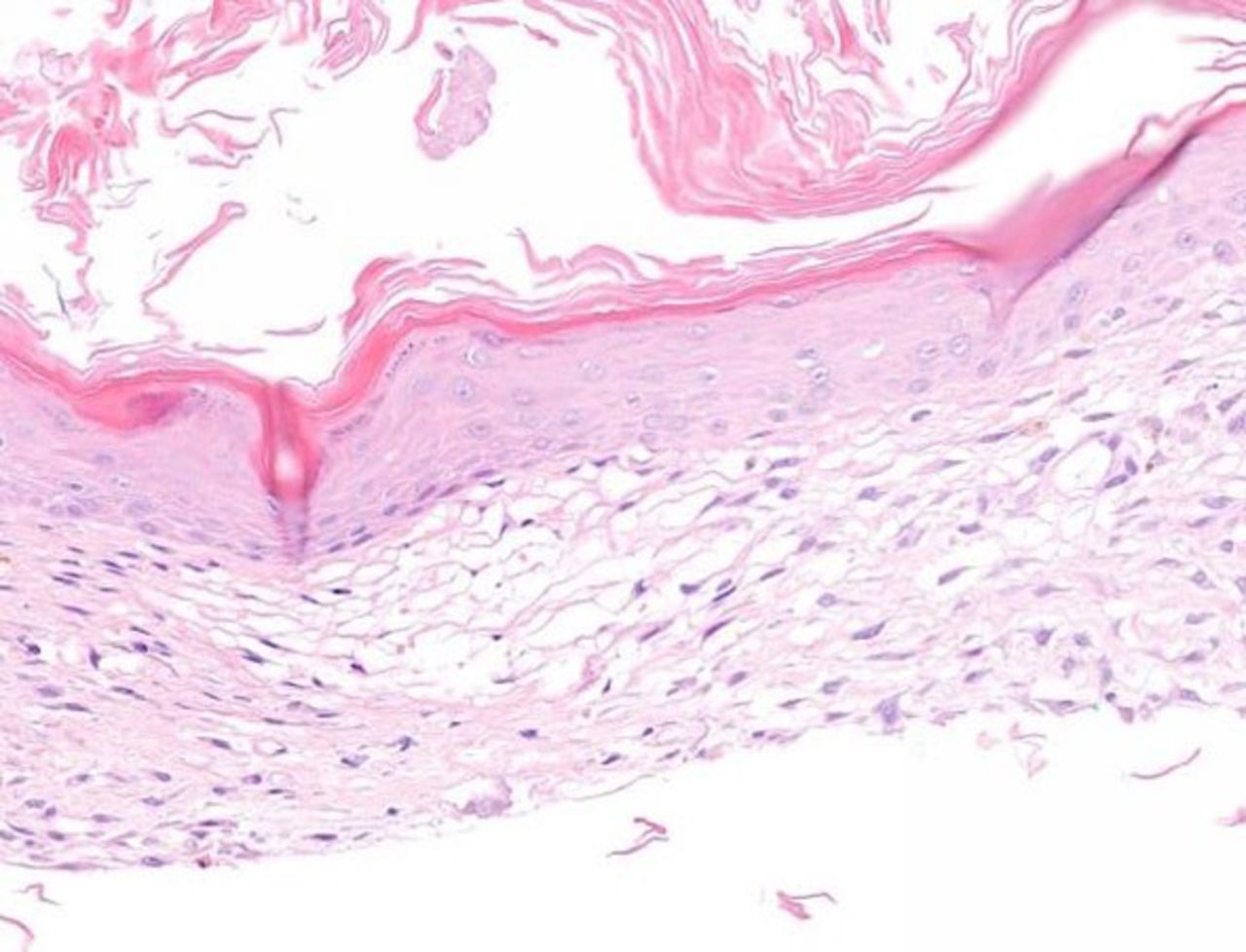
The patient was young and disturbed by the impaired hearing function as well as recurrent episodes of otitis media. Thus, a surgical treatment was recommended and desired by the patient. The surgical approach was achieved by a retroauricular incision and expansion of the bony external auditory canal. Excision of the herniated part of the right tympanic membrane was performed by an experienced surgeon. Intraoperative inspection of the middle ear revealed unremarkable mucosal tissue and an intact and mobile ossicular chain (figure 6). The defect was closed by installation of an autogenous cartilage perichondrial composite graft deriving from the concha in the sense of an underlay tympanoplasty type I (figure 7). The histological workup showed a hernia sac formed by two epithelial layers, a superficial layer of squamous epithelium and an underlying layer of fibrous cells (figures 8 and 9).

Intact ossicular chain and middle ear mucosa.

Tympanoplasty type I (underlay myringoplasty).

Histological presentation of the hernia sac of the tympanic membrane after excision and H&E staining consisting of two layers (1x).

A superficial layer of squamous cells and an underlying layer of fibrous cells (5x).
Outcome and follow-up
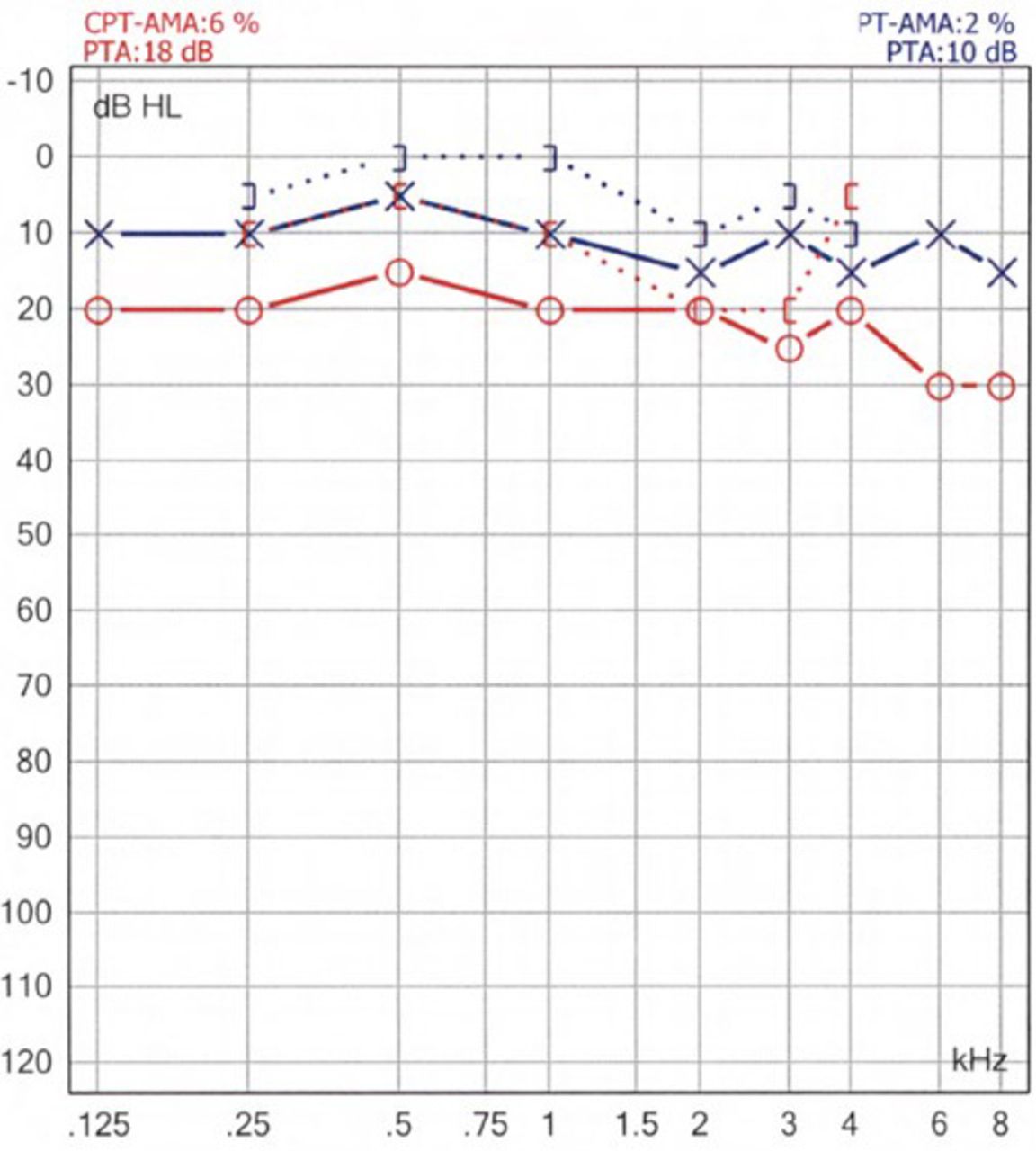
The follow-up examination 12 weeks after the surgery showed a well-healed tympanic membrane with positive Valsalva manoeuvre (figure 10). No further ear infections had been reported. The postoperative audiogram demonstrated a symmetric sensorineural hearing function and an improved conductive hearing on the affected ear. The maximum air-bone gap showed to be 10 dB HL on the right side with a reduced overall hearing loss of 6% (CPT-AMA) on the right side and 2% (PT-AMA) on the left side (figure 11). Furthermore, the satisfied patient stated an improved quality of life.

Ear microscopy 12 weeks postoperative (right ear).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Audiometry 12 weeks postoperative. CPT-AMA: Council of Physical Therapy of the American Medical Association.
Discussion
Diagnosis
Ear microscopy and patient history are guiding. Clinically, patients report about a fluctuating conductive hearing loss and sometimes tinnitus due to increased mobility of the tympanic membrane.
Habitual Valsalva manoeuvres, the so-called ‘autoinflation’ of the middle ear, will place the ossicular chain and tympanic membrane under tension and improve the transmission of sound as described by Beickert et al.9 At the present time, CT and MRI are guiding for a definitive diagnosis and useful in defining the extent and nature of bullous lesions. However, histologic analysis is sometimes necessary for exclusion of potential malignancy.10
There is no standard single test that is diagnostic for Eustachian tube dysfunction, which is considered the underlying cause. Middle ear assessments may be normal in patients experiencing chronic symptoms.11 Combinations of functional tests with patient symptomology may provide more accuracy than any single test alone.12 A validated clinical assessment is the Eustachian Tube Dysfunction Questionnaire-7.13
Pathomechanism
According to Ikeda et al, there are two conditions required for the formation of a herniation of the tympanic membrane. The first is a pre-existing defect in the pars tensa of the tympanic membrane, which, for example, occurs in otitis media with perforation or iatrogenic due to paracentesis. After remission, the second requirement is a recurrent positive pressure inside the middle ear, that can force the ‘scarred’ and thinned portion of the tympanic membrane laterally into the external ear canal.14
Positive pressure (the pulsion) inside the middle ear can lead to a transient bulging of the tympanic membrane, which is commonly encountered among patients with acute otitis media, trumpet players or after Valsalva manoeuvre. Patients who suffer from chronic otitis media with effusion often report about aural fullness. They tend to repeatedly perform Valsalva manoeuvres to create positive middle ear pressure by opening the Eustachian tube, which allows a better drainage of the fluid.15 16
Besides this method is also commonly recommended by physicians to reduce symptoms of otitis media with effusion as a low-cost and effective therapy.
Sadé described ‘hyperectasis’ of the tympanic membrane as a condition where either a small or large part of the tympanic membrane bulges above the physiological level.17
The authors of this study believe that hyperectasis is equivalent to a bulging of the tympanic membrane involving all three layers. In the presence of a pre-existing defect of the fibrous layer, excessive autoinflation can cause a herniation of the tympanic membrane.18
In this scenario, a two-layer hernia can develop through the thinned portions of the tympanic membrane.
These hernias show a higher compliance and in extreme cases, a ‘ballooning effect’ can lead to a complete occupation of the external auditory canal.
Literature review
Eustachian tube dysfunction is defined by signs and symptoms of pressure dysregulation in the middle ear such as ‘aural fullness’, ‘popping’, discomfort, pain or ‘under water sensation’11 and represents a common problem with reported incidences ranging from 0.9% to 5%.19
According to Schilder et al, the three subtypes of Eustachian tube dysfunction include barochallenge-induced dysfunction in conditions of alteration of the ambient pressure, patulous Eustachian tube dysfunction and dilatory Eustachian tube dysfunction. The latter can be broken down into functional obstruction, dynamic dysfunction due to muscular failure and anatomical obstruction.11
Acute episodes are often preceded by an upper respiratory tract infection, or exacerbation of allergic rhinitis, which causes inflammation in the Eustachian tube orifice or lumen. Chronic Eustachian tube dysfunction is defined by symptoms lasting for more than 3 months and has been associated with damage to the middle ear and the eardrum. Complications include otitis media with effusion (glue ear), middle ear atelectasis (retraction of the eardrum) and chronic otitis media with defects of the tympanic membrane.20 Consequently, it must be considered the primary cause of herniation of the tympanic membrane.11
We found the earliest mention referring to a ‘hernia of the tympanic membrane’ dating back to 4 November 1932.21 In a written protocol of a case discussion in ‘The Section of Otology’ a 24-year-old male patient was presented, who reported otorrhea from childhood up to the age of 17, which then dried up. Seven years later, the ear discharged again for several days. On examination, the right drum was red and bulging, but painless and without inflammation. Hearing by air conduction was reduced. Decades before the possibility to perform cross-sectional imaging, the authors discussed the following questions. ‘Is this a hernia of the middle layer of the drum, or is it a cholesteatoma, and if so, is the radical mastoid operation justifiable in view of the fact that the only symptom of the patient is deafness in the right ear? Should one perform paracentesis?’ They agreed on performing a conventional anteroposterior view radiography of the petrous bone, which showed no bony abnormalities. A subsequently performed paracentesis revealed ‘very thick tenacious mucus’. The final diagnosis in this case remains unknown.
According to the previous studies, the phenomenon of tympanic membrane herniation was first described and coined the term ‘pulsation hernias’ by Kwok and Hawk in a case series of adult patients in the year 1987.22 In their first case, they present a 68-year-old female patient with a history of recurrent bilateral otitis with otorrhea and a conductive hearing loss of 10–20 dB HL on both ears with increased report of the tympanic membrane. During the previous 4 years, she had experienced improved hearing after ‘autoinflation’.
The patient‘s hearing worsened after paracentesis and improved again after spontaneous healing of the tympanic membrane. No further therapy was established during a follow-up of 4 years.
Their second case is about a 44-year-old patient with a history of recurrent bilateral otitis since the age of 2. Audiometry showed a conductive hearing loss of 30 dB HL on the right side. The patient denied habitual Valsalva manoeuvres, but worked as a professional trumpet player. Initially he showed to have a herniation of the tympanic membrane, which was observed and developed into a retraction pocket after 1 year.
In the year 2001, Sadé interpreted the hyperinflated tympanic membrane as the result of an increased middle ear pressure and termed the pathology ‘hyperectasis’ in contrast to the reverse phenomenon of ‘atelectasis’. Sadé stated that positive and negative middle ear pressures are physiological phenomena that are usually buffered by a normal mastoid pneumatisation. A poorly pneumatised mastoid, however, may eventually lead to atelectasis or a hyperectatic tympanic membrane.17 Habitual nose sniffing, which can be seen as reverse Valsalva manoeuvres, will lead to a negative middle ear pressure and is related to the development of retraction-type middle ear disease, such as adhesive otitis media, secretory otitis media and cholesteatoma.23 24
In 2005, Fayad et al25 published a case report about a patient with bulging of both tympanic membranes. The 67-year-old man with hearing impairment claimed to habitually improve his hearing ability with autoinflation.
The examination showed a hearing improvement of 10–20 dB HL in high frequencies after increasing middle ear pressure by autoinflation. The authors warned that pressure equalisation tubes could worsen the situation and recommended high-frequency hearing aids.
A more severe case of a 66-year-old man with herniation of the tympanic membrane and occupation of the external ear canal similar to our case was published by Ikeda et al.14 The patient showed to have a chronic serous otitis media with left-sided conductive hearing loss and had performed habitual Valsalva manoeuvres over a course of many years. In this case, an endoscopic enaural approach was performed and a pressure equalisation tube was inserted to prevent the recurrence of a middle ear fluid collection.
Treatment
Current therapy recommendations are based on individual case reports and options depend on the extent of the bulging of the tympanic membrane. In severe cases with occlusion of the external auditory canal surgical treatment with hernia excision and tympanoplasty is generally accepted. In addition, ventilation tubes can be inserted after tympanoplasty to equalise middle ear pressure and prevent the recollection of a middle ear effusion.14
In mild cases, it is recommended to observe or suggest a reduction of Valsalva manoeuvre frequency to once a day.17 21 22
The bulging of the tympanic membrane normally diminishes or remains unchanged after conservative treatment.14 In Sadé’s case series of 59 conservatively treated patients, the membrane persisted in its hyperinflated state for weeks, months and even years. Any attempt to equalise the pressure by myringotomy or pressure equalisation tubes will only increase the conductive hearing loss and result in an unsatisfied patient.17
As Eustachian tube dysfunction must be considered the primary cause it should be addressed to prevent hernia formation in the first place and to limit postoperative recurrence of the disease. This can include medical treatment with nasal steroids, topical decongestants or antihistamines.20 Current studies suggest that surgical balloon dilation of the Eustachian tube can be a helpful therapy, although long-term data are not yet available.26
Present evidence to support its alternatives, such as laser Eustachian tuboplasty and microdebrider Eustachian tuboplasty, is limited in quantity and of poor quality.19
Although Sadé described cases of a ballooning tympanic membrane returning to its physiological level after being punctured,17 we do not recommend this approach.
Take home messages
Eustachian tube dysfunction must be considered the primary cause of herniation of the tympanic membrane.
A pre-existing defect in the pars tensa of the tympanic membrane and recurrent positive pressure inside the middle ear can lead to the formation of a two-layer hernia.
Tympanic membrane herniation is a rare benign malformation of the tympanic membrane into the external auditory canal beyond physiological levels.
Severe cases of tympanic membrane herniation are often treated with hernia excision and tympanoplasty, although recommendations are based on case studies
References
Footnotes
Contributors TE wrote this case report during his speciality training as a resident doctor in the Department of Otorhinolaryngology, Head and Neck Surgery of the Kantonsspital Aarau. It was subsequently discussed with the Head of the Department, FUM, who also contributed to the work. Literature was obtained from Pubmed. We also thank Dr. med. Roland Zweifel (Department of Pathology, Kantonsspital Aarau) for the contribution of the histological work-up.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.