Article Text

Abstract
A 26-year-old man, returned to the UK having travelled extensively in Asia. He was referred with a 3-month history of distal leg ulceration following an insect bite while in Thailand. Despite multiple courses of oral antibiotics, he developed two adjacent ulcers. A wound swab isolated an organism identified as Burkholderia thailandensis. The histology of the skin biopsy was non-specific. A diagnosis of cutaneous melioidosis was made, based on clinical and microbiological grounds. The ulcers re-epithelialised on completion of intravenous ceftazidime followed by 3 months of high dose co-trimoxazole and wound care. Many clinical microbiology laboratories have limited diagnostics for security-related organisms, with the result that B. pseudomallei, the causative bacterium of melioidosis, may be misidentified. This case highlights the importance of maintaining high levels of clinical suspicion and close microbiological liaison in individuals returning from South-East Asia and northern Australia with such symptoms.
- dermatology
- infections
- tropical medicine (infectious disease)
- wound care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Melioidosis is an infection caused by Burkholderia pseudomallei, an environmental Gram‐negative bacillus endemic in the tropics and subtropics, most commonly reported in northern Australia and Southeast Asia.1 Acquisition is via exposure to contaminated soil or surface freshwater, with transmission primarily by implantation or inhalation. A significant cause of morbidity and mortality in these regions, infection may be localised or disseminated and presentations vary from acutely fulminant to chronically indolent. Pneumonia occurs in about 50% of cases, often accompanied by bacteraemia and septic shock with mortality rates of 10%–20%. Important risk factors for severe disease are diabetes, excessive alcohol use, chronic renal and chronic lung disease but it may occur, uncommonly, in healthy individuals. Approximately 20% of individuals present with cutaneous melioidosis (CM), mostly with chronic ulcers and abscesses but CM can also be complicated by necrotising fasciitis, osteomyelitis and sepsis.2 3 In non-endemic areas, melioidosis poses a diagnostic challenge due to its ability to mimic other diseases including pulmonary tuberculosis.
This case report describes a case of CM, where the presenting complaint was non-healing leg ulceration.
Case presentation
A 26-year-old man who returned to the UK having travelled extensively in Asia was referred to our dermatology service with a 3-month history of distal left leg ulceration. He reported a lesion on the lateral left lower leg just proximal to the lateral malleolus, which he attributed to an insect bite while in Thailand. Initially, the lesion was erythematous, enlarged and subsequently ulcerated. The lesion was debrided in Nepal and then again in India. There was no improvement and despite multiple courses of oral antibiotics, he developed two more ulcers, on the anterior and medial lower leg, adjacent to the original ulcer (figure 1). The edges of the ulcers were undermined which raised the clinical suspicion of pyoderma gangrenosum. The patient was systemically well with no evidence of fever, lymphadenopathy or organ dysfunction.

Clinical photographs of the ulcers prior to treatment with intravenous ceftazidime, oral co-trimoxazole and negative pressure dressings and after.
Investigations
A full blood count, urea and electrolytes, ESR and CRP were normal. Serology tests for HIV, Schistosoma, Strongyloides, Mycoplasma and Leishmania were negative. He had a weakly positive antinuclear antibody (1:80 nucleolar) and a negative double-stranded DNA.
An MRI scan of the left leg did not demonstrate evidence of tendinopathy or osteomyelitis.
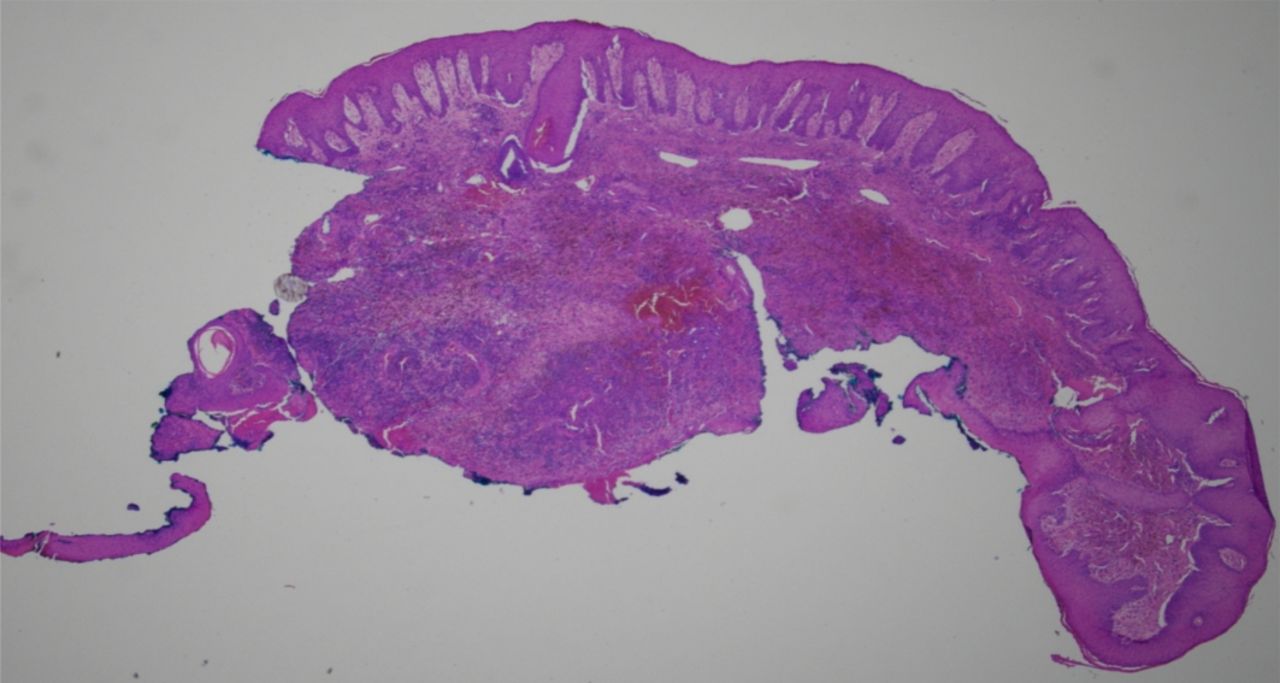
An incisional skin biopsy was taken and the histology demonstrated ulceration and an acanthotic epithelium, overlying a deep dermal inflammatory infiltrate comprising of neutrophils, lymphocytes, histiocytes and plasma cells (figure 2). There was no evidence of granulomas, vasculitis, malignancy or viral inclusions. Gram, DPAS, Grocott, Giemsa, Ziehl-Neelson and Wade-Fite special stains were all negative. The histological features were non-specific. Tissue bacterial and fungal cultures produced no significant growth, and Lesihmania PCR was negative.

{kind=link}
{kind=link}
Incisional biopsy at low power with H&E staining demonstrating ulceration on the left, adjacent to an acanthotic epithelium with a dermal inflammatory infiltrate comprising of neutrophils, lymphocytes, histiocytes and plasma cells.
After multiple wound swabs did not isolate a pathogen, one taken at the referring hospital grew an organism, which was identified as Burkholderia thailandensis.
A diagnosis of CM was made, based on clinical and microbiological grounds. The causative organism for melioidosis is B. pseudomallei. The bacterial identification methodology identified B. thailandensis, a closely related but non-pathogenic relative; however, the organism’s unusual antibiotic susceptibility profile made B. pseudomallei a more likely culprit. Unfortunately, the isolate had been discarded and so further analysis was not possible.
Differential diagnosis
The initial list of differential diagnoses for this case was wide given the non-specific presentation and patient’s extensive travel through Southeast Asia. He had travelled from Indonesia, the Philippines, Vietnam, Cambodia, Thailand, Nepal and India.
Infectious diseases were high on the list of differentials in this young fit man. Pathogens causing cutaneous ulceration most frequently include pyogenic bacteria such as Staphylococcus aureus and various beta-haemolytic streptococci. Mycobacterial infections may also produce cutaneous ulcers—Mycobacterium tuberculosis, M. ulcerans and non-tuberculous mycobacteria. Cutaneous leishmaniasis was considered, although clinical appearance and geographical exposure made this possibility unlikely. Fungal infections to consider include mycetoma, chromomycosis and sporotrichosis,4 typically after implantation injuries. These were excluded with blood, tissue cultures and special stains on histology.
He had no risk factors for venous or arterial ulceration and there was no evidence of neuropathy. The undermined edges and violaceous surrounding tissue did raise the suspicion of pyoderma gangrenosum; however, neutrophils were not a prominent feature on histology.
The skin biopsy did not demonstrate evidence of malignancy or vasculitis, important differentials in a patient with non-healing ulceration.
The possibility of melioidosis was discussed with the microbiology department when a wound swab was reported as having isolated B. thailandensis.
Treatment
The patient had an initial course of antibiotics, followed by debridement at a hospital in India. On his return to the UK, he received multiple courses of antibiotics including amoxicillin, flucloxacillin, clindamycin and co-amoxiclav with no improvement.
Intravenous ceftazidime three times a day with oral co-trimoxazole (160 mg/800 mg) one tablet two times a day was started. Fucibet cream (a combined topical potent corticosteroid and fusidic acid), along with various wound dressings were used with no significant effect.
Once a diagnosis of CM was made, the dose of co-trimoxazole was increased to the recommended (160 mg/800 mg) two tablets two times a day with folic acid supplementation for 3 months. The topical corticosteroid was stopped. Our specialist dermatology nurse debrided and dressed the wound with a negative pressure dressing on a weekly basis for several weeks. The patient was then taught how to manage the negative pressure dressing.
Outcome and follow-up
Within 3 weeks of starting the higher dose of co-trimoxazole and negative pressure dressings, the ulcers re-epithelialised with scarring (figure 1). There has been no recurrence of the skin lesions 20 months after stopping oral co-trimoxazole.
Discussion
Melioidosis is a challenging diagnosis to make. It is an important differential to consider in returning travellers with non-healing skin lesions or systemic illness. The prospective study and review of the literature carried out by Gibney et al3 demonstrated that the usual risk factors for systemic melioidosis of diabetes, alcohol excess and chronic renal and lung disease are often not present in individuals with CM. Investigations should include swabs to identify B. pseudomallei and should otherwise be guided by clinical presentation. MRI is useful to exclude osteomyelitis If there is ulceration.
Due to the inherent resistance of B. pseudomallei to multiple antibiotics, the recommended treatment regimen of soft-tissue infection comprises of two phases: an initiation period with intravenous ceftazidime or meropenem and co-trimoxazole followed by an eradication phase with oral high-dose co-trimoxazole for 3 months.5 The need for an intravenous stage in CM is uncertain, given reports of improvement in some cases with oral antibiotics alone.3
The diagnosis of melioidosis has traditionally relied on culture using selective media, biochemical tests and antibiograms that demonstrate intrinsic penicillin and aminoglycoside resistance. More recently however, laboratories have adopted matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry identification systems that examine bacterial cell proteins by their molecular weight and electronic charge. Species-specific signatures can be generated, allowing organisms to be identified by matching signatures to those in reference databases. However, many clinical microbiological laboratories do not have access to libraries that include security-related organisms, with the risk that any such organisms may be given alternative identifications. Consequently, B. pseudomallei isolates have previously been reported as the non-pathogenic B. thailandensis.6 7 In the UK, Public Health England provides a species-specific molecular service for the diagnosis of melioidosis, and to date confirm that all isolates of B. thailandensis that have been submitted to them have in fact proven to be the closely related organism B. pseudomallei (D. Kenna, personal communication). This therefore emphasises that a high clinical suspicion is key to the diagnosis of CM.
Patient’s perspective
“It all started in Thailand in December. I was staying at a hotel near a beach and noticed what I thought was an insect bite on my lower leg. It turned into a horrible black pustule which I squeezed and it formed a deep hole in my leg about 2 mm across. I carried on my travels and flew from Thailand to Nepal. I was very naive at this point and I didn’t know what an ulcer was. I even went on a 10-day hike in Nepal. However, around a month after, the ulcer had grown to around 10 mm across. I went to a doctor who gave me a minor debridement and some antibiotics. After a few months in Nepal, I carried on my travels to India where I got food poisoning. While I was unwell, I neglected to clean the wound with saline and change my bandages which I had been doing once a day. Then when I looked at it, the ulcer had a foul smell with a yellow discharge and it was surrounded by a blue ring. It looked like the skin around it was dead. I spoke to a surgeon in England who was a friend of the family. He told me I needed to get it debrided now. When I asked for the worse case scenario, he told me there was a possibilty of amputation. I was in a remote area in North India, so I travelled to a larger town, a day’s journey away. A surgeon agreed to debride the wound. This left an ulcer 35 mm in diameter and looked as if it was healing nicely. However, next to the original ulcer, the skin around it was irritated by the bandage and got infected. I then flew back to England in February and went to my GP who referred me to Dermatology at UCLH. Initially I was told it could possibly be pyoderma gangrenosum which freaked me out. I looked it up online and thought, this is something I am going to have to live with because it’s not a curable thing. At this point, the initial ulcer had started healing but two new ulcers had formed next to it, so I had three ulcers on my leg.
My practice nurse was cleaning the wound every 3 days and applying all sort of bandages, mainly aluminium based but it wasn’t improving. I was referred to a local wound care specialist who tried soaks and wipes with non-adherent gauze but the wounds didn’t change.
I went back to the GP for my results but all my blood tests were negative. No one knew what was going on. My whole leg had become swollen around the ulcers. Every morning I would lie in bed and I would dread getting up because every time I stood up, the blood would rush to the wounds and it was a sensation of knives stabbing me in the leg. It was absolutely agonising. I also had reduced mobility of my ankle so I couldn’t walk properly. It was probably the scariest time of my life. No one knew what was going on, I had expected once I got back to England it would heal but it was getting much worse and my mobility was decreasing.
After being in England for around 2 months, the nurse bandaging my leg collected some of the milky discharge which had started coming from the ulcer. That was the first sign of infection. The test showed this Burkholderia thailandensis. I was then admitted to a ward at my local hospital where I spent 3 days in isolation on intravenous antibiotics. I had so many different types. I was re-referred to UCLH with the test result and was told it was very strange for B. thailandensis and it was likely Burkholderia pseudomallei but unfortunately the hospital didn’t save the sample. The doctors were then confident in what to do and the right type of antibiotics to treat me with. I had been on them for months and felt awful with stomach problems. I was put on intravenous antibiotics three times a day at my local acute medical unit which lasted for 4 weeks and then a nurse came to my house for another 2 weeks. I wasn’t able to do anything else. I couldn’t really walk but luckily I could stay with my parents who supported me.
During this period, the amazing nurse in charge at the dermatology department of UCLH was treating my wound. She told me it was probably going to hurt and I was going to hate her for it. It was absolute agony but it really helped. She used a debriding pad and scrubbed the wound. I would see her once a week to change my dressing. I then had a special dressing with suction which she taught me how to use. That made such a difference to my wounds.
After about 6 months, the ulcers finally healed. It wasn’t until this time that I could walk normally and by August, so around 8 months later, I could run without pain. I have some pretty strange scars with discoloured rings where the ulcers were but I’ve not had any problems since they healed. I managed to do a ski season which I have always wanted to do and I’ve gone back to work in construction. I now really appreciate my health.
The thing I was not prepared for was how it affected me mentally. It was really trying. I never considered how a physical illness can cause such a mental battle. Looking back, it makes me feel emotional. I am blessed to have had the support of my family and the NHS for all the care I had.”
Learning points
Cutaneous melioidosis is an important differential diagnosis to consider in a returning traveller from Southeast Asia and northern Australia.
Many UK laboratories may not have access to the extended database required to identify Burkholderia pseudomallei and so high clinical suspicion is needed and referral to a tertiary centre may be required.
Optimal treatment for cutaneous melioidosis remains uncertain but may include intravenous therapy with ceftazidime or meropenem in addition to a prolonged oral course of co-trimoxazole.
Ethics statements
Acknowledgments
Dr Peter Ellery Consultant Microbiologist, University College London Hospitals NHS Foundation Trust, Department of Microbiology, London, UK, peter.ellery@nhs.net. Oana Olarasu Senior Staff Nurse, University College London Hospitals NHS Foundation Trust, Department of Dermatology, London, UK. oana.olarasu@nhs.net.
Footnotes
Contributors CS contributed to compiling clinical details, writing report and conducting the interview with the patient for their perspective. OV contributed to compiling clinical details and reviewing the report. SM-J contributed to writing and reviewing the report. SLW contributed to compiling the clinical details, writing and reviewing the report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.