Article Text

Statistics from Altmetric.com
- cardiovascular medicine
- drugs and medicines
- gastroenterology
- general practice / family medicine
- unwanted effects / adverse reactions
Description
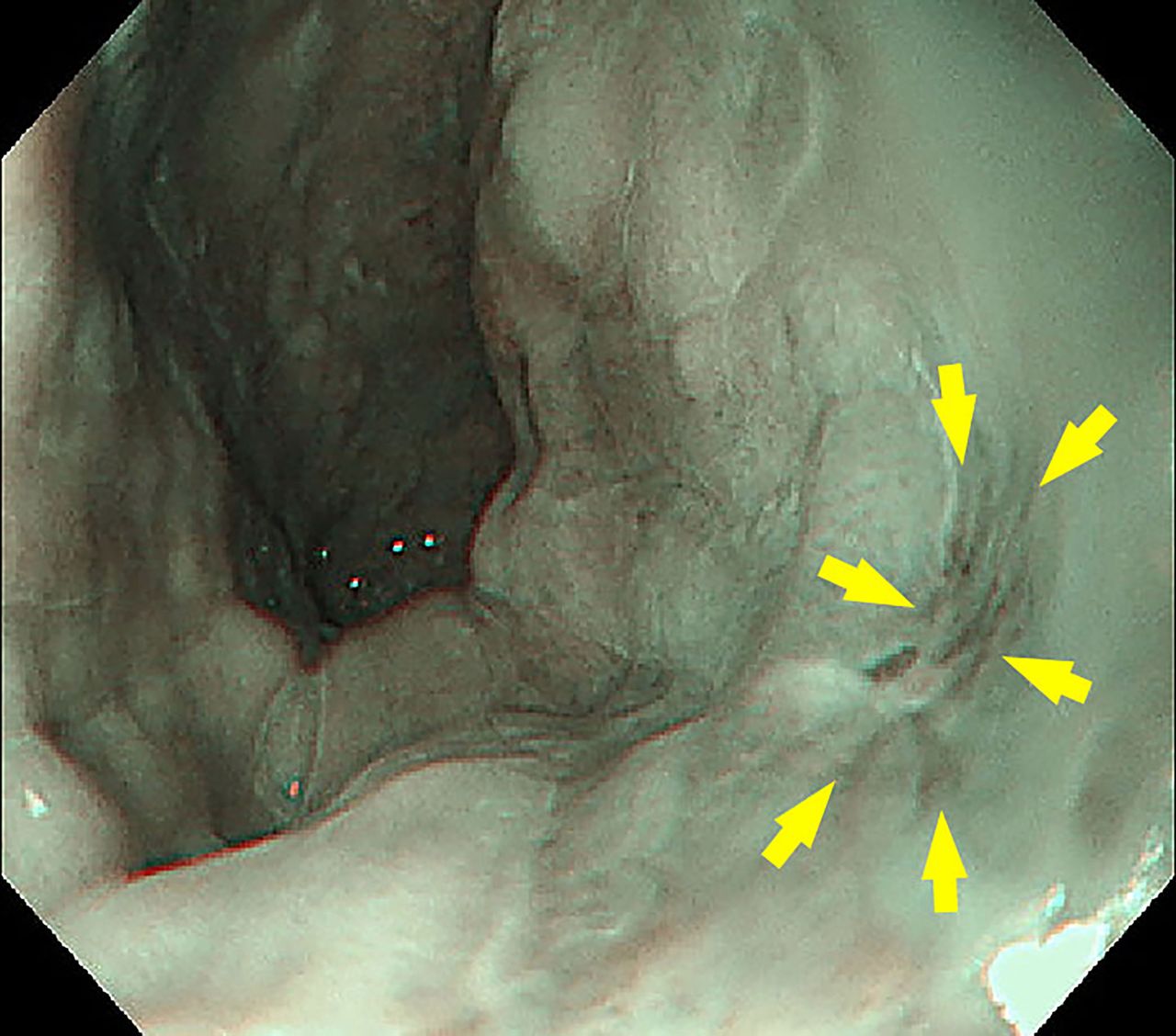
An 85-year-old man presented to our clinic with chest discomfort for a month while swallowing solids. His symptoms did not change with posture. He had experienced no change in body weight. His medical history revealed hypertension, type 2 diabetes mellitus and paroxysmal atrial fibrillation, for which he had been prescribed oral doses of 80 mg/day of telmisartan, 1000 mg/day of metformin, 2.5 mg/day of bisoprolol, 100 mg/day of diltiazem hydrochloride and 220 mg/day of dabigatran etexilate. His vital signs were unremarkable. Laboratory tests showed no abnormalities. One week later, an oesophagogastroduodenoscopy showed erosions in the lower oesophagus (figure 1). The biopsy of the lesions revealed no remarkable findings other than mild inflammatory cell infiltration into the epithelium.

{kind=link}
Oesophagogastroduodenoscopy showed erosions in the lower oesophagus.
Because drugs could cause oesophagitis, we further investigated his medication history thoroughly. It revealed that the direct oral anticoagulant (DOAC) had been switched from apixaban to dabigatran 2 months before when the doctor in charge of management of paroxysmal atrial fibrillation changed from a cardiologist at a general hospital to his family doctor. He took dabigatran with a large amount of water as his family doctor instructed. However, he used to lie down immediately after consuming the medication. Therefore, we considered dabigatran-induced oesophagitis (DIE). His oral medication was reverted to apixaban, and his condition improved in a few days.
Various drugs have been shown to cause oesophagitis, including non-steroidal anti-inflammatory drugs, quinidine, doxycycline, tetracycline, clindamycin, ideocyclin, oxytetral ferrous sulfate, ascorbic acid, alprenolol chloride, theophylline, mycophenolate mofetil, warfarin, cyproterone acetate, ethinylestradiol, rifampin, cefotiam hydrochloride, phenytoin and dabigatran.1 Toya et al reported that DIE occurred in 21% of patients who took dabigatran1; furthermore, in the reviewed literature, no cases of oesophagitis induced by DOACs other than dabigatran have been reported.1 Dabigatran is prescribed as a relatively large capsule (18–19 mm in length, 280–390 mg in weight), which can easily get lodged in the oesophagus.2 It is reported that the size and weight of the capsule affect the oesophageal transit time, and capsules are more likely to adhere to the oesophageal mucosa compared with tablets.2 3 Therefore, dabigatran has a tendency to get lodged in the oesophagus.2 Dabigatran is the only DOAC containing the eluting tartaric acid core, which can cause oesophageal injury.2 Because dabigatran can dissolve in a strongly acidic environment, it has tartaric acid as the core, which is coated with dabigatran etexilate.2 The pH of tartaric acid is 2.4; a significantly acidic environment is created.2 Instructing patients to take dabigatran orally with a large amount of water and to maintain an upright position for a while after taking it have been reported as effective ways to prevent dabigatran from lodging in the oesophagus.2 For patients who cannot continue taking dabigatran due to side effects, switching to another DOAC may be an effective way to improve gastrointestinal symptoms.
Learning points
Oesophagitis occurs in 21% of patients who took dabigatran; furthermore, in the reviewed literature, no cases of oesophagitis induced by direct oral anticoagulant (DOACs) other than dabigatran have been reported.
Dabigatran is the only DOAC containing the eluting tartaric acid core that can cause oesophageal injury. Because dabigatran can dissolve in a strongly acidic environment, it has tartaric acid as the core, which is coated with dabigatran etexilate.
Patients who cannot continue taking dabigatran due to side effects such as oesophagitis, switching to another DOAC may be effective to improve gastrointestinal symptoms.
Ethics statements
Footnotes
Contributors KI identified the significance of the case and wrote the manuscript, and DY, TM and MI revised it. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.