Article Text

Description
Granular cell tumour (GCT) is an uncommon but usually benign lesion of neural/Schwann origin. This tumour type is most frequently found in skin, subcutaneous tissue and oral cavity, mostly in black middle-aged women.1 This lesion type can involve any organ, including the gastrointestinal (GI) tract. The appendicular involvement though is extremely rare.
We report a case of a pregnant female patient in her early 30s who went to the emergency department after 2 days of enduring persistent pelvic pain. The blood tests indicated leucocytosis, neutrophilia and elevated C reactive protein concentration.
Abdominal ultrasound examination revealed an outer appendiceal diameter of 8 mm, with a markedly thickened and stratified wall. The increased density of the surrounding fat tissue was consistent with phlegmon.
A laparoscopic appendectomy was performed.
Careful gross examination showed that the appendix was increased in size, the appendiceal wall was markedly thickened and the lumen filled with faecal material.
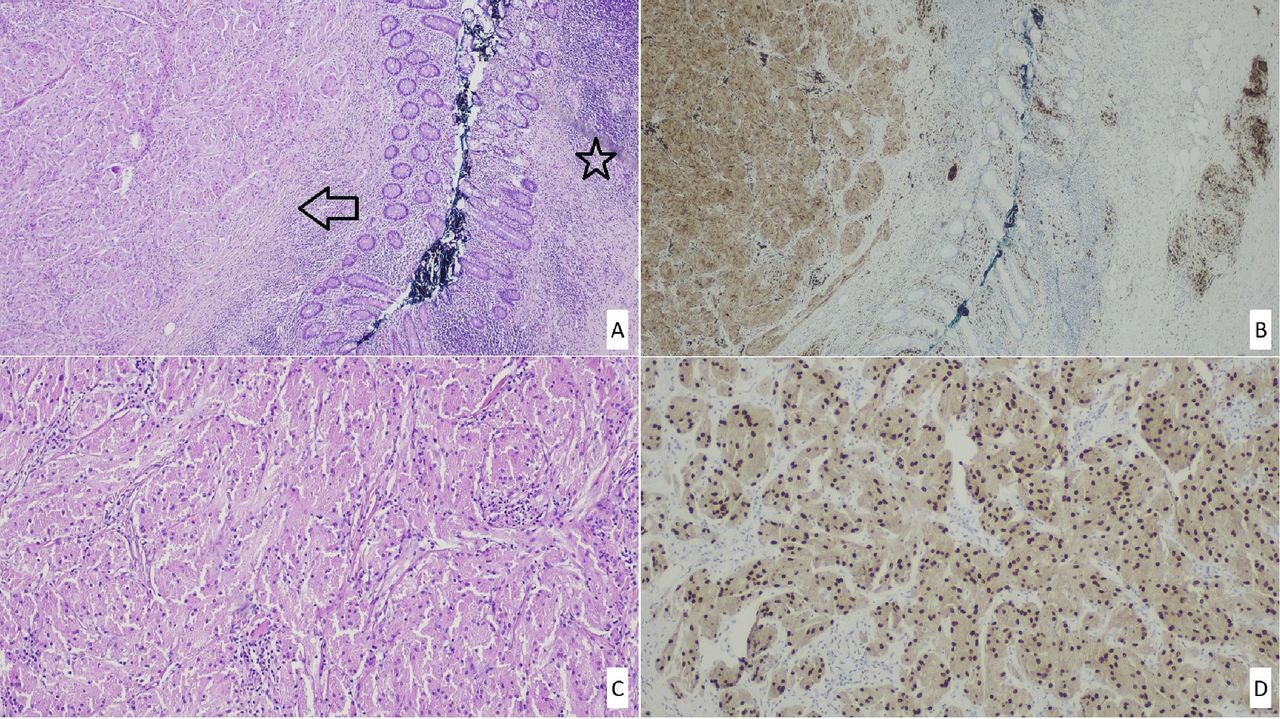
The complete histological analysis of the specimen revealed a well-circumscribed and unencapsulated nodule with 0.5 cm in diameter confined to the submucosa. There was also a florid granulomatous chronic inflammation measuring 1.2 cm extending to the tip of the appendix (as shown in figure 1A). This granulomatous inflammation was located in the wall and involved its entire thickness, except the overlying mucosa. The multiple, coalescent microgranulomas (non-necrosing granulomas) were composed only of epithelioid histiocytes. The authors want to emphasise that there was no clinical or imaging procedure of the thorax, which may constitute evidence for tuberculosis diagnosis. The surrounding tissues showed reactive and hyperplastic mucosa, with no atrophy. There were no acute appendicitis lesions.

{kind=link}
(A) Submucosal GCT (arrow) was contiguous with a chronic granulomatous inflammation zone (star), (H&E, ×20). (B) The tumour cells and granulomas without necrosis found in the appendix wall were immunoreactive for CD68. (C) The round to oval tumour cells displayed a granular cytoplasm (H&E, ×100). (D) The neoplastic cells typically expressed nuclear SOX-10 (×100). GCT, granular cell tumour.
The nodule was composed of nests of epithelioid cells with abundant granular eosinophilic cytoplasm and central small round nuclei (as shown in figure 1C). The tumour was devoid of cytological atypia and necrosis.
Immunohistochemistry revealed S-100 protein strong and diffuse positivity, suggestive of Schwann cell origin, and it was not expressed by the granulomatous epithelioid cells. The GCT cells also displayed SOX-10 nuclear expression (as shown in figure 1D) and CD68 membrane expression. CD68 pointed out to the granulomas found in the appendix wall (as shown in figure 1B).
The postoperative period was uneventful, and the patient was discharged after 1 week.
Less than 15% of GCTs occur in the GI tract, with only 15 cases being reported in the appendix so far.1 2
A detailed analysis (table 1) of the features of GCTs in the appendix reveals that the male/female ratio was 1:1, the mean age was that of 41 years old and the average size of the lesions was 1.4 cm. The patients’ clinical characteristics, including from the patient reported in this article, can be consulted in table 1.
Clinical characteristics of patients reported in the literature with GCT of the appendix
The pathogenesis of GCTs remains unclear; however, the medical literature data suggest that a chronic inflammation, surrounding the GCT, is an antecedent condition that may favour its appearance.
In fact, chronic and unresolved inflammation promotes immunosuppression and so it has been associated with an increased risk of developing both benign and malignant tumours.
Furthermore, published reports indicate that GCT in the appendix is a lesion which reflects local reactive changes of the neural/Schwann cells rather than a true neoplasm.3
This case documents a GCT probably arising from a granulomatous appendicitis background, which is a rare entity. This chronic inflammation corresponds to less than 2% of appendectomies as a cause of appendicitis.
Surgical intervention with wide local excision and complete resection is still the best treatment for GCTs in the GI tract, with excellent outcomes for benign lesions and with a low rate of recurrence or malignant transformation.
There are no data in the literature that correlate with the emergence of GCT in the lower GI tract and the risk of developing colorectal cancer.
Previous reports suggest that regardless of the initial nature of the lesion, all patients should be followed to prevent recurrence and distant metastasis.
Learning points
Granular cell tumour (GCT) is an uncommon benign lesion of neural/Schwann origin.
The appendicular involvement is extremely rare.
We report a case of granulomatous appendicitis and a GCT as an incidental finding, whose symptoms and analytical parameters mimic an appendicitis.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors JIMM and RCO—drafting and revision of preliminary and final versions, and approval of the final version. MRS and MAC—histology, revision of preliminary and final versions, and approval of the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.