Article Text

Statistics from Altmetric.com
Description
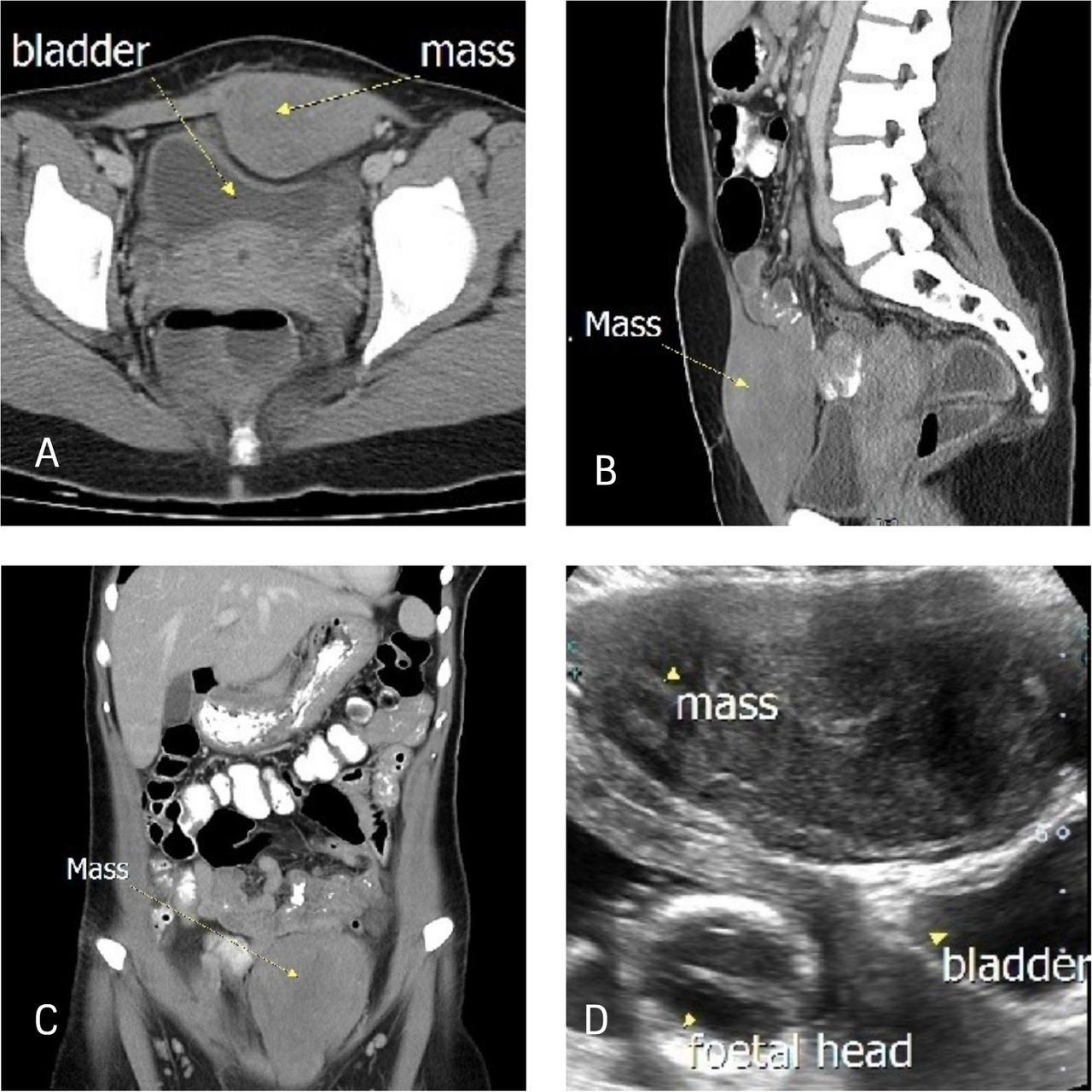
A woman in her late 20s, gravida 2 para 1 at 13 weeks pregnancy with a history of caesarean section, presented with a rapidly growing abdominal mass around the site of the caesarean scar. Prepregnancy CT scan showed an intramuscular solid mass in the left rectus abdominis measuring 4×7×10 cm and another subcutaneous mass at right hypochondrium measuring 2×4×5 cm (figure 1A–C). Histopathological examination from tru-cut biopsies confirmed ‘desmoid-type fibromatosis’. Although she did not have any history of familial adenomatous polyposis, subsequent gastrointestinal surveys were suggestive of Gardner’s syndrome with presence of multiple colonic polyps. Other extraintestinal manifestations of Gardner’s syndrome like epidermoid cysts, dental abnormalities, osteomas and tumours of other organs were not evident. Subsequently, she was lost to follow-up for until she became pregnant again.

CT scan: axial (A), sagittal (B) and coronal (C) views showing the mass repressing and pushing the bladder posteriorly, and ultrasound showing the relationship of the mass, bladder and the fetus (D).
During pregnancy, the progressively enlarging mass was associated with troublesome lower urinary tract symptoms (LUTS). Clinically, a left suprapubic mass measuring 15×12 cm and a right hypochondriac mass measuring 5×5 cm were felt (figure 2A). On ultrasound, the suprapubic mass was seen repressing onto the pelvic organs with bladder and lower uterus being pushed posteriorly (figure 1D).

{kind=link}
{kind=link}
Demarcation of the abdominal wall masses (A), midline skin incision away from the masses (B), mass obstructing access to the lower uterine segment (C) and the repaired classical uterine incision (D).
She was managed conservatively during pregnancy and planned for surgery following delivery. Even though the current management policy for desmoid tumour is active surveillance, surgery is deemed necessary in this patient in view of her symptoms and poor follow-up compliance. Elective caesarean section was decided as the mode of delivery in view of the risk of obstructed labour. Bilateral tubal ligation was advised as future pregnancy might impair the flexibility of the repaired abdominal wall and may endanger the health of both mother and fetus.1
Due to worsening LUTS with advancing gestation, an elective caesarean delivery was performed at 34 weeks. At caesarean section, an upper midline laparotomy approach was performed away from the mass and a classical uterine incision was chosen to deliver the baby as the mass was limiting the surgical field and obstructing access to the lower uterine segment (figure 2B–D).
Both mother and baby were well after delivery and her case was transferred to the care of gastrointestinal and plastic surgeons. Prophylactic colectomy was advised in view of significant future risk of colorectal malignancy in Gardner’s syndrome, which she has yet to agree. Few months after delivery, she underwent wide local excision with mesh abdominoplasty which cured her symptoms.
Learning points
Desmoid abdominal wall tumour in pregnancy is a rare event.
The time and mode of delivery in such cases should be individualised, depending on the associated symptoms and the site of the tumour.
A suitable surgical incision during caesarean section must be adopted to avoid incision onto the tumour mass and, if the lower uterine segment is inaccessible, a classical upper segment uterine incision is required.
Subsequent pregnancy is not advised in patients with huge desmoid tumour with a large abdominal wall defect following definitive surgery.
Ethics statements
Patient consent for publication
Acknowledgments
We wish to thank our gastrointestinal surgeon, Mr Mohd Fadliyazid who co-managed this case and critically appraised our manuscript.
Footnotes
Contributors NMS wrote the manuscript, FMD reported the CT scan and ultrasound findings, MSBMH was involved in the preoperative discussion and subsequent operation and RR was involved in the preoperative discussion, performed the operation and edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.