Article Text

Statistics from Altmetric.com
- Liver disease
- Tropical medicine (infectious disease)
- Infection (gastroenterology)
- Foodborne infections
- Hepatitis and other GI infections
Description
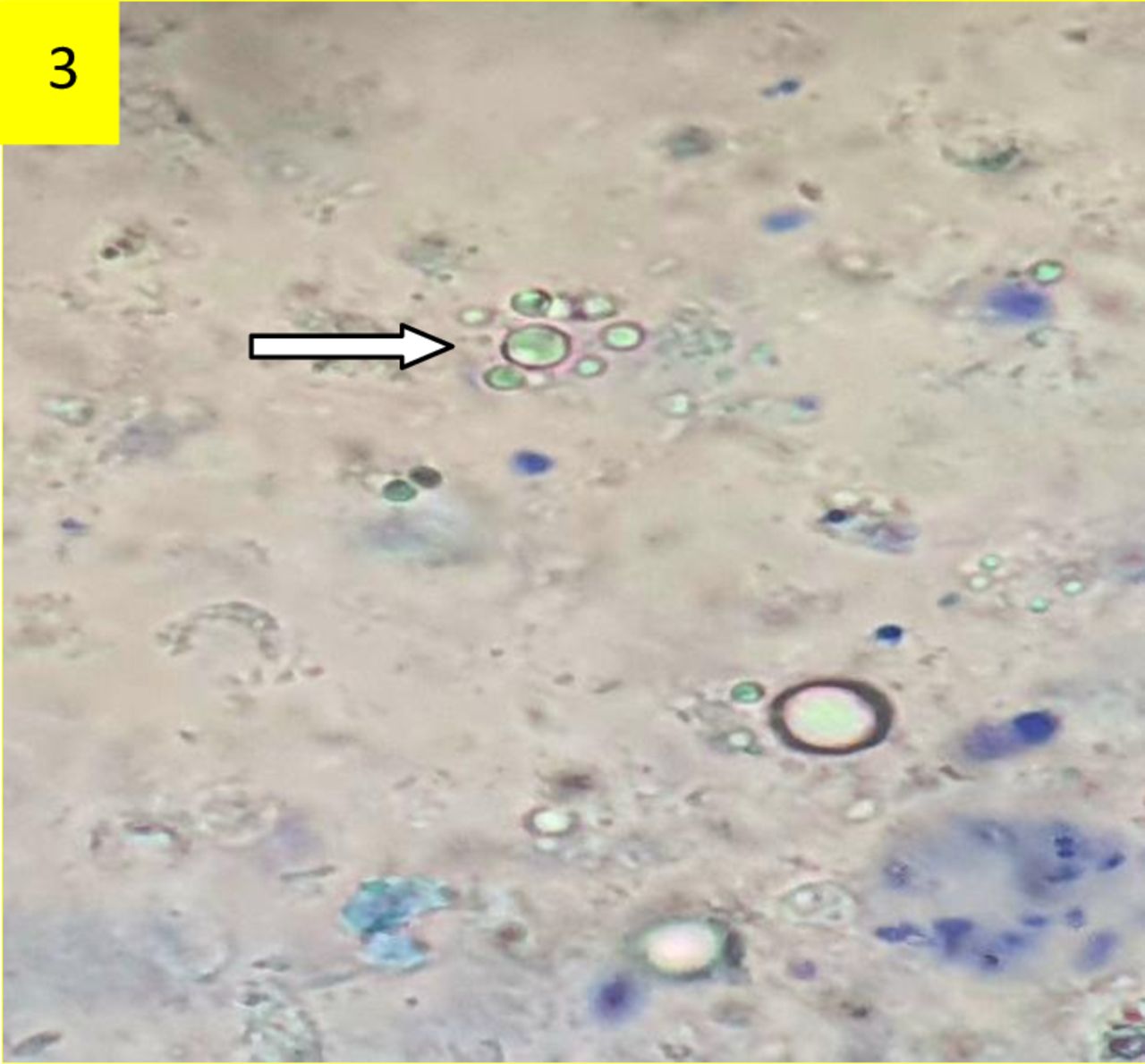
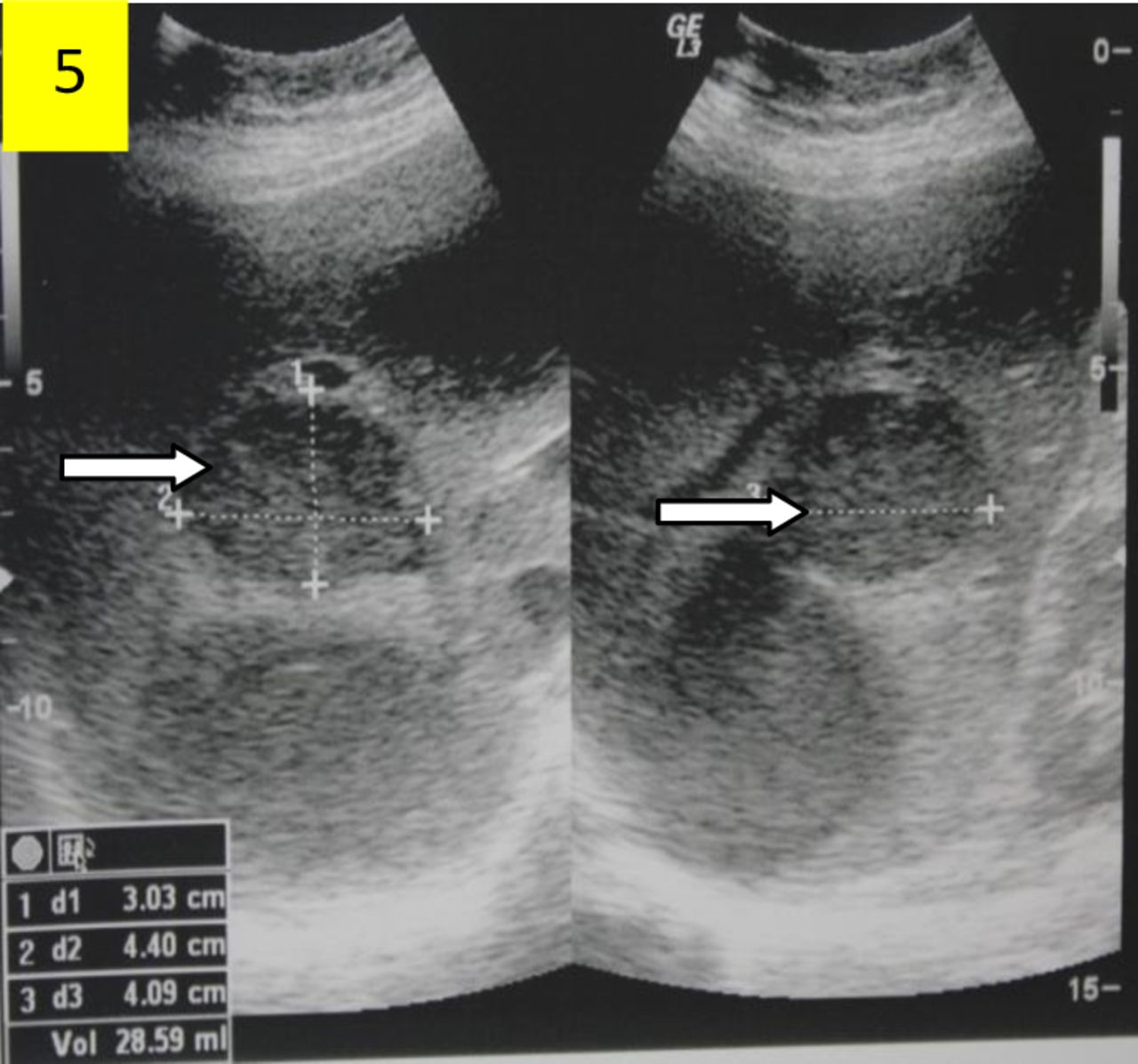
A female patient in her 60s, with no known comorbidities, presented with a 3 month history of low-grade fever and persistent fatigue. She also exhibited anorexia and a weight loss of 4 kg during the same period. The patient reported no symptoms of cough, nausea and vomiting, abdominal pain, difficulty in urination, bloody stools or worm infestation. Her personal history was unremarkable. On examination, she appeared pale, and an enlarged tender liver was palpable during abdominal examination. Laboratory tests showed a haemoglobin level of 89 g/L (reference range 130–150 g/L) and a normal total leucocyte count. Liver and renal function tests were unremarkable. Subsequently, the contrast-enhanced computed tomography (CECT) of the abdomen revealed hepatomegaly with multiple hypo-dense lesions involving liver segments IVa (7 × 5 cm), IVb (7 × 5.4 cm), VII (7.5 × 8 cm) and VIII (7.5 × 4.2 cm) displaying imperceptible walls and most lesions extended until the subcapsular aspect of the liver (figure 1). The aspiration of two large liver lesions yielded 300 mL of viscous anchovy sauce-like fluid (figure 2). Due to the aspirate’s colour, an amoebic liver abscess was suspected, and intravenous metronidazole treatment was initiated empirically. Amoebic serology returned positive results with a serum IgG index of 3.73 against a normal index of 0.9. Microscopic analysis of the aspirate revealed trophozoite forms of Entamoeba histolytica (figures 3 and 4). However, stool microscopy for Entamoeba histolytica proved to be negative on two separate occasions. A definitive diagnosis of amoebic liver abscess was made on the basis of strong clinical suspicion, radiographic, microscopic and serological evidence. The patient showed good therapeutic response following 2 weeks of antiamoebic medication and 1 week of lumicidal therapy (tablet nitazoxanide 500 mg two times per day). The ultrasonography (USG) abdomen after treatment revealed a dramatic improvement in lesions compared with the USG abdomen before treatment (figure 5).

Contrast-enhanced computed tomography (CECT) abdomen reveals multiple low attenuation lesions with peripheral rim enhancement involving various liver segments (white arrows).

Test tube and sample container showing thick anchovy sauce-like aspirate from liver.

Direct microscopic examination of fluid aspirate. Photomicrograph (40×) showing few scattered trophozoite forms of Entamoeba histolytica admixed with few scattered pus cells and occasional red blood cells.

Direct microscopic examination of fluid aspirate. Photomicrograph (40×) showing trophozoite forms of Entamoeba histolytica with ingested erythrocytes, 3 to 4 nuclei and centrally placed karyosome.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ultrasonography (USG) abdomen shows reduction in size of abscess after 2 weeks of anti-amoebic therapy (white arrows).
Discussion
Amoebic liver abscess (ALA) predominantly affects males between 30 and 60 years of age.1 In contrast to pyogenic liver abscess (PLA), ALA typically manifests as a solitary lesion, with the right hepatic lobe being the primary site of involvement; however, the left lobe and multifocal patterns may also be seen.2 The aspirate from ALA is often devoid of inflammatory cells due to apoptotic hepatocytes, while pyogenic abscesses contain purulent material.3 PLA is characterised by a foul odour, in contrast to the odourless, viscous and dark brown amoebic aspirate, commonly referred to as anchovy paste—a distinctive feature of this specific abscess.4 Diagnostic methods include microscopic examination, serological testing and imaging techniques. Antibodies against Entamoeba histolytica can be identified in 92–99% of cases; however, negative test results may occur during the initial week of illness. Trophozoites are present in only 20% of aspirates when the cyst wall specimens are acquired.4 5 Fine needle aspirate culture is the preferred diagnostic approach for PLA rather than ALA. On ultrasound, ALA lesions appear as round, well-defined, hypoechoic, cystic masses that generally cannot be distinguished from other aetiologies of liver abscess.2 Standard treatment comprises antiamoebic therapy (eg, metronidazole) followed by a luminal agent administration such as paromomycin or nitazoxanide to eliminate intestinal cysts.5
Learning points
The amoebic liver abscess is a significant consideration in the differential diagnosis of fever of unknown origin, particularly in the elderly population, and warrants thorough investigation.
Amoebic liver abscess typically manifests as a right hepatic lobe solitary lesion, although it may also be present in the left lobe and exhibit a multifocal pattern.
The identification of parasites in bodily fluids or tissue samples by microscopic inspection is the gold standard in the diagnosis of amoebic liver abscess.
Ethics statements
Patient consent for publication
Acknowledgments
Authors would like to express special thanks to Dr Sibi E, Radiologist at Military Hospital Golconda, Hyderabad(India) for the valuable guidance and support in completing this case report
Footnotes
Contributors The following authors were directly involved in the patient’s care: BA, RV, AS. The following authors were not directly involved in the patient’s care, they contributed to the manuscript: TAV. The following author is the clinician in charge of the clinical care of the patient, who supervised the preparation of the manuscript, was responsible for obtaining informed consent from the patient/guardian/family members and is responsible for the overall integrity of the content of the manuscript: BA. TAV helped in manuscript editing. The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content: BA, RV, AS, TAV. The following authors gave final approval of the manuscript: BA, RV, AS, TAV.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.