Article Text

Statistics from Altmetric.com
Description
A man in his 80s with a history of hypertension and dementia presented to the emergency department with acute encephalopathy attributed to euvolaemic hyponatremia. Admission vitals documented a blood pressure of 147/45 mm Hg with a pulse pressure (PP) of 102 mm Hg; otherwise, his initial admission note did not document any abnormal cardiovascular physical examination findings. On morning rounds, the general medicine team observed exaggerated visible distension and collapse of the bilateral carotid arteries (online supplemental video 1). The finding, known as Corrigan’s pulse, indicates chronic aortic valvular regurgitation (AR).1 The wide PP and Corrigan’s pulse prompted the examiner to reposition the patient to an upright sitting and forward leaning position in order to move the heart closer to the chest wall and increase the audibility of a potential AR murmur.2 A blowing III/VI, decrescendo diastolic murmur was present along the left upper sternal border, the typical murmur of chronic AR.1 A laterally displaced point of maximal impulse (PMI) was present, but other peripheral findings of AR or signs of congestive heart failure were absent.
Supplementary video
Corrigan’s pulse was first defined by Dr D J Corrigan in April 1832 in The Edinburgh Medical and Surgical Journal article, ‘On Permanent Patency of the Mouth of the Aorta, or Inadequacy of the Aortic Valves’. He described ‘visible pulsation of the arteries of the head and superior extremities…[which] are suddenly thrown from their bed, bounding up under the skin’.3 Dr Corrigan observed that this finding results from the large stroke volume followed by the exaggerated collapse of the large vessels on the diastolic return of blood to the left ventricle and, thus, loss of diastolic distention of the large vessels when AR is present (figures 1 and 2).3 4

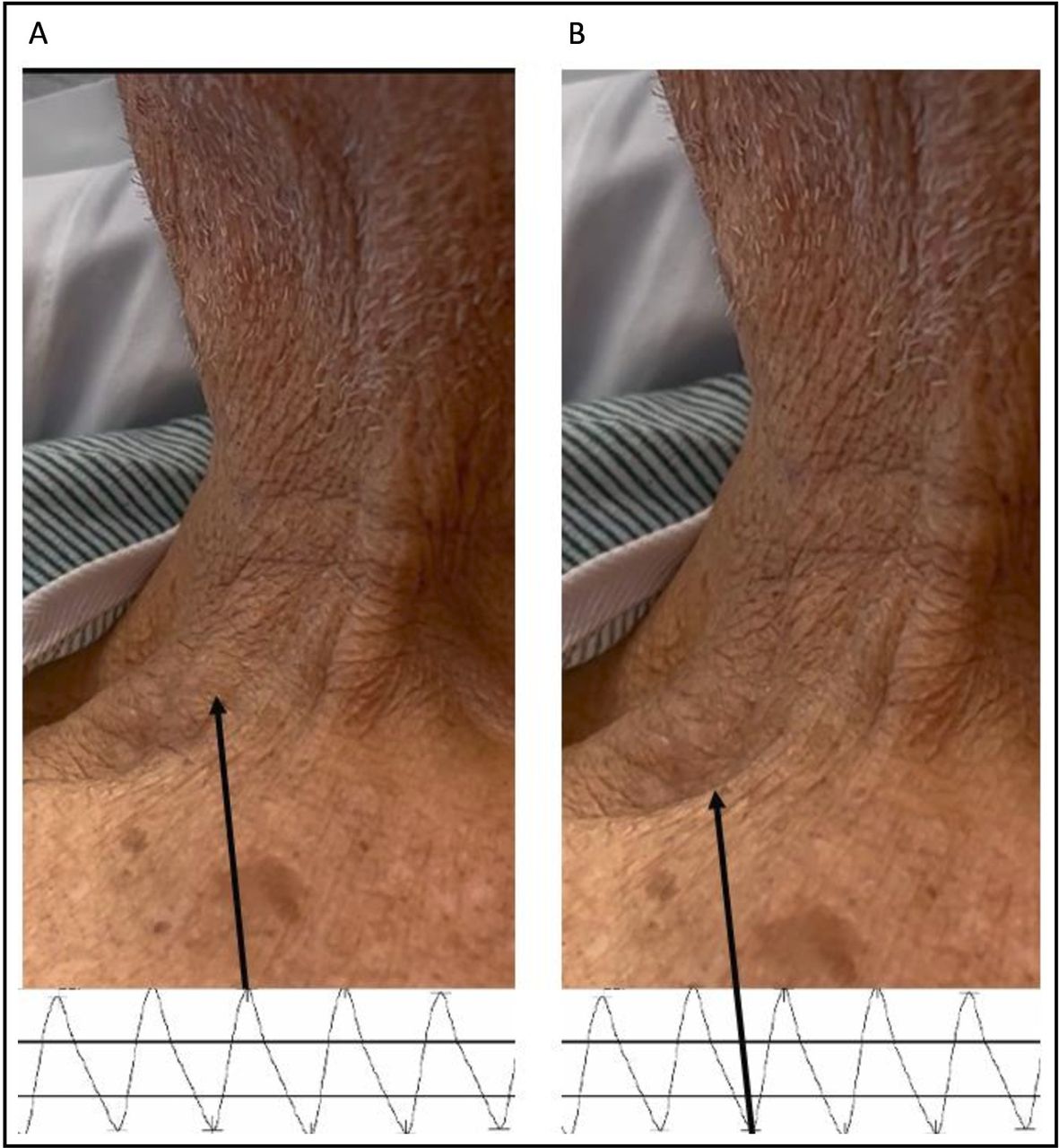
Still images from online supplemental video 1 showing rapid systolic upstroke (A) and subsequent diastolic collapse (B) of the carotid artery in our patient with chronic AR. Corresponding aortic waveform tracings indicate the phase of the cardiac cycle during which these findings occur (pressure tracing from a separate patient with chronic AR). AR, aortic valvular regurgitation.

{kind=link}
{kind=link}
Examples of what might be expected on an aortic waveform tracing from the cardiac catheterisation of (A) a patient with normal cardiac cycle and (B) a patient with severe, chronic AR (separate patient from online supplemental video 1). What is seen at the bedside in a patient with Corrigan’s pulse is the marked contrast between the high stroke volume and quick carotid upstroke followed by a rapid decline in arterial pressure during diastole, indicated by the wide PP. AR, aortic valvular regurgitation; DBP, diastolic blood pressure; PP, pulse pressure; SBP, systolic blood pressure.
Observing Corrigan’s pulse prompted the examiner to appropriately position the patient to best auscultate the murmur of AR. The classic diastolic murmur increases the probability of AR (likelihood ratio (LR) = 9.9), providing a pretest probability of 41% for moderate to severe AR.1 The positive LR of moderate to severe AR with diastolic blood pressure (DBP) of ≤50 mm Hg and PP of 80 mm Hg is 19.3 and 10.9, respectively. Therefore, the post-test probability of moderate to severe AR with a DBP of 45 mm Hg was greater than 90% prior to a transthoracic echocardiogram. The location of the murmur, peripheral pulse findings and wide PP were atypical of other valvular heart diseases causing diastolic murmurs such as mitral stenosis or pulmonic regurgitation.
The medical team presented diagnostic and management options to the patient and family. The patient’s family members declined further evaluation, including transthoracic echocardiography, and instead opted for clinical surveillance, citing his advanced dementia and physical disability due to osteoarthritis rather than cardiopulmonary symptoms.
Corrigan’s pulse and other peripheral pulse findings, while unreliable predictors of AR severity, should prompt a more detailed cardiovascular evaluation and can reveal clinical exam findings highly predictable of AR.1 5 Frequently, AR can be diagnosed with appropriate bedside manoeuvres, direct observation and Bayesian reasoning based on these exam findings rather than pursuing further diagnostic testing.
Learning points
Corrigan’s pulse is a distinctive clinical exam finding for chronic aortic valvular regurgitation (AR).
Corrigan’s pulse results from rapid distension of the large vessels followed by exaggerated diastolic collapse due to loss of diastolic distention of the large vessels as blood regurgitates from the aorta into the left ventricle.
When the typical diastolic murmur is present, a diastolic blood pressure of ≤50 mm Hg and a pulse pressure of ≥80 mm Hg increase the probability of moderate to severe AR.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TJ contributed to direct patient care, acquiring the images and writing the manuscript. JMC participated in direct patient care, acquiring the images and consent, and provided critical revisions and final approval of the submitted draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.