Article Text

Abstract
Junctional ectopic tachycardia (JET) is a relatively uncommon arrhythmia predominantly observed in infancy, often occurring after congenital heart surgery. Although JET is rare in adults, it can occur in the presence of myocardial ischaemia. We describe a woman in her early 70s who presented with multivessel ST-segment elevation myocardial infarction and underwent percutaneous coronary intervention on left anterior descending artery and right coronary artery. She developed JET on the second day, resulting in haemodynamic compromise. Despite initial treatment attempts including amiodarone and beta-blocking agents proving insufficient in controlling JET, we successfully managed by administering ivabradine. Subsequently, she was discharged with recovered cardiac function without recurrence of JET. JET often proves refractory to multiple antiarrhythmic agents and can lead to unfavourable outcomes. Several case reports have demonstrated the effectiveness of ivabradine in treating JET during infancy, which can also be an effective therapeutic option for adult without adversely affecting haemodynamics.
- Ischaemic heart disease
- Arrhythmias
- Interventional cardiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Junctional ectopic tachycardia (JET) is an uncommon tachyarrhythmia characterised by abnormal automaticity at the atrioventricular (AV) node or proximal His bundle, resulting in AV dyssynchrony and often resistance to antiarrhythmic therapy.1 While JET is rare in adults, it can manifest in specific pathological conditions including myocardial ischaemia.2 Under conditions of reduced contractility in both ventricles, JET can have a pronounced haemodynamic impact due to the loss of AV synchrony and rapid ventricular rates. We present a rare case of JET complicated by ST-segment elevation myocardial infarction (STEMI) and demonstrate the efficacy of ivabradine in its management.
Case presentation
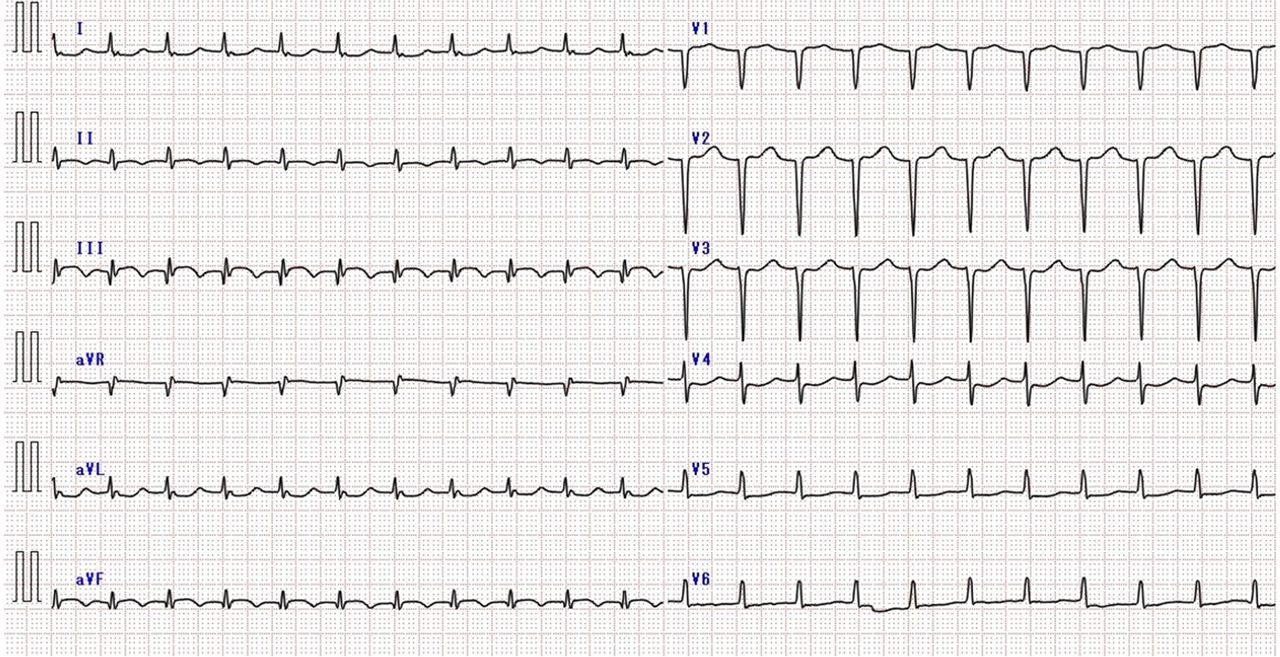
A woman in her early 70s presented to the emergency department with a 10-day history of progressive chest pain. She had no comorbidities, medications and was a non-smoker. The only cardiovascular risk factor was a family history of ischaemic heart disease. On arrival, blood pressure (BP) was 121/66 mm Hg, but heart rate (HR) was elevated at 130–140 beats/min. The ECG showed sinus tachycardia with ST-elevation in leads III, aVF, and V2-6, and Q waves in leads V1-6 (figure 1). Transthoracic echocardiography revealed severe hypokinesia of the anteroseptal and inferior walls of the left ventricle, accompanied by a significant reduction in left ventricular ejection fraction (LVEF) of 15%–20%. Laboratory tests showed elevated levels of creatine kinase (CK), CK-MB, high-sensitivity troponin T (10 925 pg/mL; normal range<14 pg/mL) and lactate (4.25 mmol/L; normal range 0.5–2.2 mmol/L), indicating circulatory failure. Her condition gradually deteriorated with BP dropping to 90/60 mm Hg, accompanied by dyspnoea and oxygen desaturation. We diagnosed multivessel STEMI and immediately performed an emergent coronary angiography (CAG), which revealed severe stenotic lesion in the left anterior descending artery (LAD) and occlusion in the proximal right coronary artery (RCA) (figure 2). Left ventricular mechanical support using a transvalvular, microaxial flow device (Impella CP, Abiomed, Danvers, Massachusetts, USA) and mechanical ventilation were started prior to revascularisation due to dropped BP to 61/41 mm Hg after CAG. Successful primary percutaneous coronary intervention (PCI) was performed for both the RCA and LAD to achieve complete revascularisation.

The 12-lead ECG on admission showed sinus tachycardia with ST-elevation in leads III, aVF, and V2-6, and Q waves in leads V1-6.

The initial coronary angiography identified occlusion in the proximal RCA ((A)—arrowheads), and critical stenotic lesion in the proximal and mid LAD ((B, C)—arrowheads). An Impella CP assist device was inserted (arrows in (D–F)), and an emergency PCI was performed, deploying DES in both the LAD and RCA, resulting in successful revascularisation (D–F). DES, drug-eluting stents; LAD, left anterior descending artery; PCI, percutaneous coronary intervention; RCA, right coronary artery.
On the second day, the patient developed narrow QRS tachycardia, accompanied by a drop in BP (figure 3 and asterisk in figure 4). Paroxysmal supraventricular tachycardia was suspected, and ATP was administered. However, the arrhythmia was only transiently suppressed and re-emerged shortly thereafter (dagger in figure 4). Despite various attempts to manage the tachyarrhythmia, involving the correction of electrolyte imbalances such as magnesium sulphate, discontinuation of catecholamine agonists, rapid infusion of amiodarone, and administration of a beta-blocking agent (landiolol), the patient persistently transitioned between sinus rhythm (SR) and tachyarrhythmia. While the cardiac index (CI) had recovered up to 2.8 L/min/m² (normal range at rest 2.6–4.2 L/min/m²) prior to the onset of the arrhythmia, this circumstance led to a significant decrease in BP (by 20–30 mm Hg) and CI (by 0.7 to 1.0 L/min/m²).

The 12-lead ECG on the second day showed narrow QRS tachycardia.

Clinical coarse on acute phase. Emergence of narrow QRS tachycardia (asterisk). Repetition of sinus rhythm and narrow QRS tachycardia (dagger). Conduction of electrophysiological study (double dagger). Insertion of atrial overdrive pacing lead through coronary sinus (section). Start of ivabradine administration (double pipe). BP, blood pressure; CI, cardiac index; HR, heart rate.
On the third day, an electrophysiological study was conducted to differentially diagnose and assess the treatability of this arrhythmia through catheter ablation (CA) (double dagger in figure 4). Consequently, the earliest activation site of this tachyarrhythmia was identified at the His bundle. Analysis of the tachycardia initiation pattern revealed variations in the His-His intervals leading to subsequent atrial–atrial (A-A) variations, suggesting dependence on the AV node and excluding the possibility of atrial tachycardia. Furthermore, right ventricular premature stimulation at the refractory period of the His bundle failed to reset the subsequent A-A intervals, confirming the absence of a concealed accessory pathway. On returning to SR, the pattern demonstrated a gradual decrease in HR and spontaneous restoration (figure 5). Thus, JET was diagnosed rather than re-entry arrhythmias. CA for JET carried the risk of AV block, necessitating consideration of permanent pacemaker implantation. We chose to persist with medical therapy employing amiodarone and landiolol; however, JET remained insufficiently suppressed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Electrophysiological study. Heart rate during junctional ectopic tachycardia (135 beats/min) was a slight increase compared with sinus rhythm (123 beats/min).
On the fourth day, we introduced an atrial overdrive-pacing lead through the coronary sinus (CS) at a slightly elevated HR compared with that observed during JET, aiming to preserve AV synchrony and suppress JET (section in figure 4). While the decrease in BP and CI associated with JET showed some improvement with the recovery of cardiac function, the patient continued to experience recurrent episodes of JET and SR transitions when CS pacing was discontinued. Increasing the doses of amiodarone or landiolol proved challenging due to hypotension, necessitating an alternative method to suppress JET in order to eventually wean off CS pacing and Impella CP. Referring to several reports demonstrating the efficacy of ivabradine in treating JET in infancy, we chose to use ivabradine to pharmacologically suppress on the sixth day (double pipe in figure 4). JET was completely suppressed with this approach without affecting the patient’s BP or CI. Consequently, the patient’s haemodynamic status was well controlled, allowing for the removal of Impella on the seventh day and CS pacing lead on the 12th day. Amiodarone was discontinued on the 19th day due to QT prolongation, yet no recurrence of JET was observed.
Outcome and follow-up
A follow-up echocardiogram revealed a significant recovery in LVEF to 50%–55%. The patient was discharged on the 36th day, and non-eventful during a 10-month follow-up period, including JET recurrence.
Discussion
JET can be classified based on its aetiology, including congenital, postoperative and focal paroxysmal and non-paroxysmal forms.3 Focal JET, which often affects older children and adults, can manifest as either paroxysmal or non-paroxysmal forms. Non-paroxysmal JET is more common in adults and characterised by a gradual onset and termination with HR of 70–130 beats/min. It is associated with myocardial ischaemia, digoxin toxicity, chronic obstructive pulmonary disease, rheumatic carditis, electrolyte imbalances and post-cardiac surgery.1 The potential mechanisms underlying focal JET involve increased automaticity within AV node or triggered activity due to delayed posterior depolarization.4 The clinical course of adult JET is generally considered non-malignant and similar to other forms of supraventricular tachycardia. However, in our case, the compromised function of both ventricles, the loss of AV synchrony and rapid ventricular rates had a significant impact on haemodynamics despite a modest increase in HR during JET compared with SR. Treatments for JET typically involve deep sedation, correction of electrolyte imbalances, discontinuation of catecholamine agonists, mechanical ventilation, fever avoidance and surface cooling. If these protocols prove ineffective, a combination of atrial overdrive-pacing, pharmacotherapy and hypothermia can be considered.2 In cases where JET remains refractory to these treatments, CA of the focal site can be an option. However, it is important to note that a recent multicentre study reported a high recurrence rate (53%) and a significant risk of AV block (21.4%) following CA of idiopathic JET in adults.5
Ivabradine act by selectively inhibiting hyperpolarisation-activated cyclic nucleotide-gated channels, primarily in the sinus node and also in the AV node. This action leads to a reduction in the pacemaker I(f) (‘funny’) current, resulting in a slowing of the diastolic depolarization gradient and a decrease in automaticity. Consequently, the automaticity of the AV junction is suppressed, which is believed to be effective in treating JET.
Several retrospective reports have demonstrated successful conversion of postoperative JET using ivabradine as an adjunctive therapy.6–8 Moreover, a randomised trial has shown the non-inferiority of ivabradine to amiodarone as a prior monotherapy for managing postoperative JET in children, establishing the usefulness of ivabradine in this context.9 Additionally, ivabradine has a relatively haemodynamically neutral profile compared with many alternative antiarrhythmic agents, as evidenced by cohort and randomised, double-blind, placebo-controlled trials in children with dilated cardiomyopathy, which showed the safety of oral ivabradine therapy without adverse effects.10 In our case, despite JET complicated by cardiogenic shock following STEMI proving insufficient to conventional therapies, ivabradine demonstrated an additional therapy without adversely affecting the haemodynamics.
Patient’s perspective
I don’t remember when I came to the hospital. I don’t remember ever having chest pains, but I think there was something wrong with me. Also, my pulse had always been fast.
My family told me that I had been in a very difficult situation during my hospital stay. My family was carefully briefed by the doctor on my condition and told that I was receiving the latest treatments. I am very grateful for the excellent care I was received. I have been making the most of every day since I got out of the hospital.
Learning points
Although junctional ectopic tachycardia (JET) is rare in adults, myocardial ischaemia can occasionally lead to the development of JET.
Under conditions of reduced contractility in both ventricles, JET can have a pronounced haemodynamic impact due to the loss of atrioventricular synchrony and rapid ventricular rate.
The utilisation of ivabradine could prove to be an effective alternative in adult patients experiencing JET, particularly in situations where the escalation of amiodarone or beta-blocking agent dosages is restricted by low blood pressure or cardiac index, all without inducing noteworthy haemodynamic compromise.
Ethics statements
Patient consent for publication
Footnotes
Contributors YN was responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content. TO, TN and HO gave final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.