Article Text

Abstract
This case reviews the clinical course of an elderly woman on chronic total parenteral nutrition who developed sepsis secondary to a rare, newly described gram-negative rod known as Phytobacter ursingii. The patient noticed a leak in her Hickman catheter when infusing her nutrition. 24 hours after a new catheter was replaced, the patient developed fevers, chills and weakness. She presented to the hospital with hypotension and tachycardia, meeting shock criteria. Blood cultures grew P. ursingii, and the diagnosis of septic shock was confirmed. Susceptibilities informed antibiotic coverage, and she ultimately improved within the next 48 hours.
- Nosocomial infections
- Adult intensive care
- Parenteral / enteral feeding
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Phytobacter ursingii is a rarely encountered bacterium first categorised within the Enterobacteriaceae family in 2018.1 Since the discovery of the Phytobacter genus in 2008, there has been a growing body of evidence that species within this genus, mainly P. diazothrophicus, play a role in opportunistic nosocomial infections.2–4 Currently, there are no published case reports describing P. ursingii infection. However, retrospective genomic analysis has confirmed P. ursingii’s presence in a prior sepsis outbreak of contaminated intravenous fluids in 1972 and showed its potential misidentification as Pantoea agglomerans in prior outbreaks.4 This report serves to describe the first case of P. ursingii sepsis that was identified at the time of illness and may serve as a basis for the literature on clinical features, antibiotic susceptibility, prognosis for sepsis and microbiological identification pitfalls with this bacterium in the adult age group.
Case presentation
A woman in her 80s called into the hospital’s interventional radiology department because there was a hole in the Hickman catheter that she used for infusing total parenteral nutrition (TPN). The patient had a history of atrial fibrillation, hypothyroidism, chronic heart failure with reduced ejection fraction, anxiety and short-gut syndrome secondary to complicated caecal volvulus requiring multiple bowel resections and ileostomy. As a result, she had been on daily TPN infusions for 6 years prior to this presentation. The leakage made her unable to receive her nutrition, and the patient was advised to go to her local emergency department (ED) for intravenous fluids. They scheduled a catheter exchange for 24 hours later at our hospital.
On the morning of her planned catheter exchange, she described feelings of fatigue, unsteadiness, headaches and leg cramps. She went to a local ED where vital signs, electrolytes and liver function tests were normal. Her white blood cell (WBC) count was 7.1 x 109 cells/L (reference range 3.7 x 109 cells/L–10.5 x 109 cells/L) with 87% neutrophils. No blood cultures were drawn as the patient’s presentation was thought to be secondary to hypovolaemia alone. The patient was given 600 mL of normal saline, which resolved her symptoms. She then came to our hospital for the scheduled outpatient catheter exchange, which was successful (figure 1).

Timeline of the patient’s clinical course. ANC, absolute neutrophil count; BUN, blood urea nitrogen; ED, emergency department; GNRs, gram-negative rods; HD, hospital day; ICU, intensive care unit; WBC, white blood cell.
Approximately 20 hours after the placement of the new catheter, the patient began to experience headache, fevers up to 38.8°C and chills. She presented to our hospital’s advanced nutrition clinic and experienced a syncopal event when standing to be weighed. She was promptly taken to the ED and was hypotensive with systolic blood pressures in the 70s (mm Hg). Physical examination was notable only for dry mucous membranes and a Hickman catheter without surrounding erythema. Laboratory studies showed a lactate of 2.8 mmol/L (reference range 0.5–1.8 mmol/L), a WBC count of 19 100/mm3 (78% neutrophils), a C reactive protein of 8.7 mg/dL (reference range 0–1.0 mg/dL), a creatinine of 1.51 mg/dL (reference range 0.67–1.17 mg/dL) and a blood urea nitrogen (BUN) of 43 mg/dL (reference range 10–20 mg/dL). Her chest X-ray and urinalysis were normal. Two sets of blood cultures, one from the catheter and one from a peripheral venipuncture, were obtained prior to administration of antibiotics.
In the ED, the patient was started on intravenous cefepime (2 g daily) and given a loading dose of vancomycin. While at a blood pressure of 75/41, she was given 2 L of normal saline with no change in her blood pressure; thus, norepinephrine was initiated, and the patient was admitted to the medical intensive care unit (ICU) for treatment of shock. Over the next 48 hours, the patient demonstrated marked improvement, with down-titration and ultimate discontinuation of norepinephrine on day 3 of hospitalisation.
12 hours after the blood cultures were drawn, growth was observed in four of four culture bottles, confirming the diagnosis of distributive shock secondary to sepsis (no time to positivity differential between draw sites). The gram stain showed gram-negative rods, but no organism was identified by the Rapid Accelerate Pheno System, a fluorescence in situ hybridisation technology that tests for a panel of common bloodstream pathogens. Vancomycin was discontinued and the infectious disease service was consulted. While catheter tip cultures are considered part of the gold standard for confirmation of central line-associated bloodstream infections, their diagnostic and therapeutic value has come into question.5 Given the cogent source of bacteraemia (related to Hickman removal/leak), four of four peripheral cultures growing bacteria and the decision to remove the new Hickman catheter regardless of tip culture results, the infectious disease team did not obtain these cultures. The skin surrounding the catheter remained dry, intact and non-erythematous. Hickman removal was performed on hospital day 3 with interventional radiology, and subsequent blood cultures were negative.
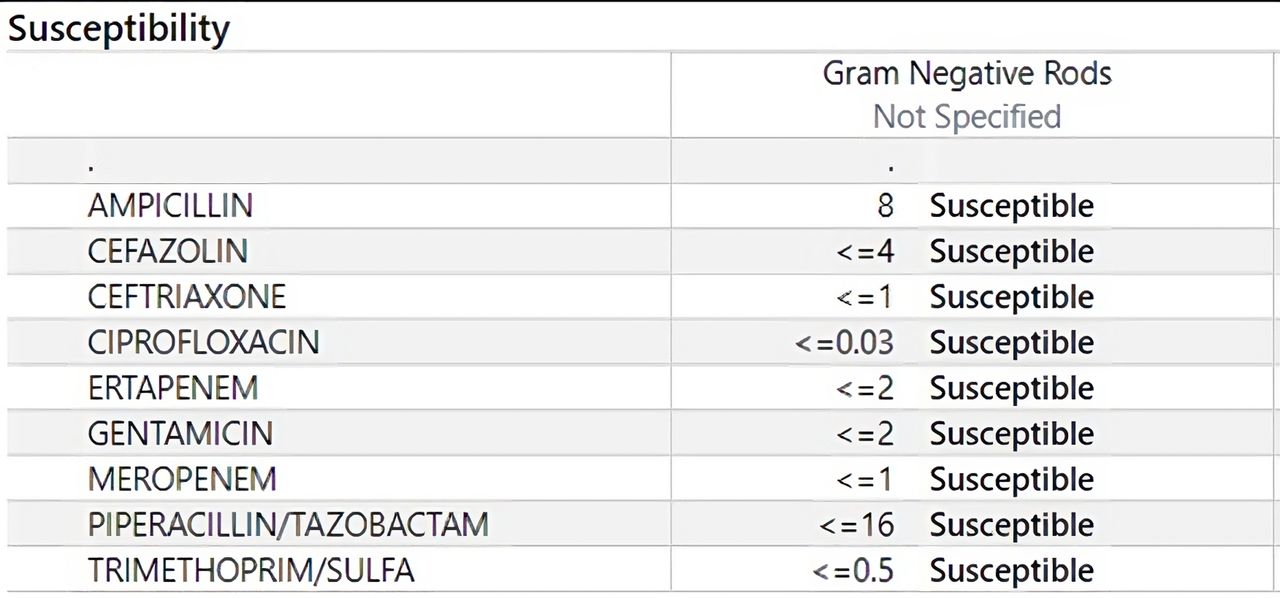
On hospital day 3, the admission blood cultures speciated as P. ursingii using the Bruker Sirius Matrix-Assisted Laser Desorption/Ionization Time of Flight (MALDI-ToF) system, and research-use-only database 11897, validated for clinical use (2022). On monotherapy cefepime, the patient clinically improved. Her WBC count lowered to 12 100/mm3, her lactate normalised to 1.3 mmol/L, BUN 29 mg/dL and creatinine had improved to 0.83 mg/dL. Enterobacteriaceae susceptibility breakpoints were used in this testing and yielded pan-sensitivity (figure 2). As a result, the patient was transitioned to ceftriaxone. On hospital day 7, after 72 hours of clear blood cultures, a new Hickman catheter was placed and TPN was restarted. The patient was discharged on hospital day 8, with a planned total course of 14 days of intravenous antibiotic therapy.

Antibiotic susceptibilities of Phytobacter ursingii strain isolated in four of four blood cultures. Enterobacteriaceae breakpoints used.
Differential diagnosis
The diagnosis of gram-negative septic shock was well supported by an elevated WBC count, signs of end-organ damage and positive gram-negative stain on blood culture. What is harder to discern is the aetiology of the introduction of the bacteria into the patient’s bloodstream.
Her symptoms the morning of her catheter replacement were likely secondary to dehydration from 2 days without TPN. However, the relative leucocytosis (baseline 3.5 x 109 cells/L) with neutrophilia seen on her complete blood count may represent the early stages of septicaemia from environmental contamination through the leaking Hickman catheter. Since no blood cultures were drawn at the time, it is difficult to confirm this. Translocation may have occurred from procedural contamination during the patient’s Hickman replacement later that day. Finally, the clinicians noted that P. ursingii and another species within its genus, P. diazotrophicus, had been retrospectively implicated as the causative pathogens in sepsis outbreaks from contaminated intravenous fluids and contaminated TPN, respectively.4 This was discussed between the head of hospital epidemiology as well as the microbiological laboratory staff but deemed extremely unlikely given the 0.2 µm filters in the TPN bags and modern intravenous fluid sterility protocols. No attempts to culture intravenous fluid or the patient’s TPN were performed.
Given the ubiquity of gram-negative bacteria in the environment, environmental contamination (procedural or via compromise of the device) remains the most compelling aetiology of bacterial inoculation.
Outcome and follow-up
The patient was discharged on hospital day 8, with a planned total course of 14 days of antimicrobials from clearance of bloodstream and removal of the Hickman catheter. This was accomplished with ceftriaxone. She was unfortunately admitted to a local hospital 2 days later with shortness of breath. There was initial concern for pneumonia, so she received 1 day of levofloxacin and vancomycin, followed by 3 days of cefepime. No blood cultures grew P. ursingii, and her clinical picture was determined to be most consistent with a congestive heart failure exacerbation. The patient was discharged on hospital day 4 after diuresis to finish her prior course of antibiotics. She has completed her ceftriaxone and is now doing well.
The patient received only 2 L total of resuscitative crystalloid in her 3-day ICU stay, and 1.6 L/day of her peripheral nutrition. By discharge, intake and outputs had shown that she had a net gain of 2 L of fluid. However, the patient was not on diuretics at home, clinically euvolaemic and asymptomatic; thus, the decision was made to discharge the patient without diuretics. Gentle diuresis prior to discharge may have prevented subsequent rehospitalisation.
Discussion
The genus of Phytobacter was originally defined in 2008, with the first species, P. diazotrophicus, found on wild rice in China and classified as Enterobacteriaceae.6 Its association with human disease was first described in a 2018 retrospective analysis of preserved bacterial strains, showing that multiple Brazilian sepsis outbreaks in 2010, 2013 and 2015 were likely caused by P. diazotrophicus.1 This analysis additionally delineated a new species within the genus, P. ursingii, which had been retrospectively identified from human sputum, a perirectal swab and contaminated intravenous fluids from a 1972 sepsis outbreak in the USA.
Since this clarification, there has been a growing body of primary evidence that species within this genus, mainly P. diazotrophicus, have played a role in multidrug-resistant nosocomial infections.2–4 Despite this emerging understanding of P. diazotrophicus, there are currently no case reports describing P. ursingii infection. This paucity of data may be representative of the difficulties of correct organism identification, more so than a lack of P. ursingii infections.4 Misidentification of Phytobacter spp is a known issue, with retrospective genotypical analysis of strains in GenBank having shown Phytobacter misclassified as Metakosakonia, Kluyvera, Enterobacter, Pantoea, Citrobacter and Enterobacteriaceae spp.3 Commonly employed phenotypical identification methods in clinical laboratories often misrepresent Phytobacter isolates as Pantoea spp, with as many as 100 reported Pantoae cases currently in question of being misidentified Phytobacter.4 With retrospective correction of a handful of these errant identifications, at present, P. ursingii has been confirmed to be isolated from sputum, gut, pancreatic cyst, hospital wastewater, soil, rectum and intravenous fluid samples, with unpublished results additionally having isolates from urine and blood. In this case, we were able to confirm the identity as P. ursingii through use of a MALDI-ToF database updated in 2022 with validated P. ursingii strains.
MALDI-ToF mass spectrometry (MALDI-ToF-MS) is a method of microorganism identification that has been growing in popularity within the last decade in the clinical laboratory. The process involves ionisation of particles within a given sample, separation by mass-to-charge ratio and measurement of the ionised particles by their time of flight to the detector. This creates a characteristic spectrum (mass-to-charge ratio on the x axis, intensity on the y axis) that can be compared with databases of known biological spectra to identify gram-positive, gram-negative, aerobic and anaerobic bacteria, as well as mycobacteria, yeast and moulds. Benefits of the method include greater accuracy of speciation compared with phenotypical or biochemical testing, smaller sample sizes needed for testing, better identification of rare organisms, easier identification of organisms with slow doubling times or complex nutritional needs, and increased speed of speciation, on average decreasing time to speciation by a full 24 hours.7 The main limitation to MALDI-ToF-MS is that identification requires comparison with known spectra included within a MALDI-ToF database. It has been shown that lack of inclusion of certain rare pathogens may lead to misidentification of samples, and consistent database updates are used to combat this issue. As databases continue to expand, the more timely and accurate diagnosis of microorganisms through the use of MALDI-ToF-MS will likely lead to its spread further throughout the field of clinical microbiology.
For the clinician, correct identification of the pathogen and aetiology of infection are paramount to preventing delays in recognition of a nosocomial outbreak, as well as delays in optimising antibacterial treatment. The only confirmed, published case of infection from P. ursingii remains the 1972 sepsis outbreak in the USA from contaminated intravenous fluid, which was only retrospectively identified 40 years later. As discussed in the ifferential diagnosis section, our patient’s infection most likely resulted from environmental contamination of the patient’s catheter, whether through device compromise or during its replacement. There is precedent for contaminated TPN and intravenous fluids to transmit Phytobacter, but this remains unlikely in our patient’s case given modern filtration and intravenous fluid sterility protocols. Given the prior intravenous fluid outbreak, isolation from hospital wastewater and the known role of another species within the genus, P. diazotrophicus, previously causing nosocomial outbreaks in at-risk populations (chronic indwelling lines, neonatal ICU patients), we surmise that P. ursingii may act similarly; however, this remains speculation. We recommend that clinicians keep a high index of suspicion for P. ursingii if Pantoea or Kluyvera spp are reported on phenotypical assays or MALDI-TOF-MS. In the case of phenotypical assays, further biochemical testing as described by Smits et al 4 can be performed to help distinguish between Phytobacter and other similar species (figure 3). Additionally, care needs to be taken to assess whether MALDI-TOF databases have been updated with Phytobacter strains, as misidentification can still occur with infrequently updated databases.

{kind=link}
{kind=link}
{kind=link}
Phenotypical characterisation of Phytobacter spp (columns 1–4, bold) and related organisms as reported by (analytical profile index) API20e test strips. 1: P. diazotrophicus (n=14); 2: P. ursingii (n=6); 3: P. palmae (n=1); 4: P. massiliensis JC163T; 5: Escherichia coli DSM 30083 T; 6: Citrobacter amalonaticus CCUG 4860 T; 7: Kluyvera intermedia DSM 4581 T; 8: Pantoea agglomerans ATCC 27155 T. Data from Smits et al 4 experiments (1–3) or from BacDive (https://bacdive.dsmz.de/) (4–8). Differences from the majority are highlighted in blue.H2S = Hydrogen Sulfide, NO2 = Nitrate Reduction Test, DSM = Deutsche Sammlung von Mikroorganismen und Zellkulturen, CCUG = Culture Collection University of Gothenburg, ATCC = American Type Culture Collection
Regarding treatment strategies, as the patient presented with undifferentiated septic shock, the mainstay of treatment was empirical cefepime and vancomycin, with intravenous fluids and norepinephrine for blood pressure support. In our case, speciation was not confirmed until hospital day 3, at which point the patient had significantly recovered on cefepime. Antibiotic susceptibility tests have never been run on P. ursingii; however, genetic analysis of known strains has shown 5 of 11 of P. ursingii strains have bacterial-resistance genes in the form of carbapenemases and extended-spectrum beta-lactamases (ESBLs).4 Despite the reported possibility of ESBL-resistance genes, we continued with cefepime given clinical recovery while awaiting susceptibility testing. Antibiotic susceptibilities showed pan-sensitive bacteria (figure 2), and the patient was successfully narrowed to ceftriaxone.
The emergence of multidrug-resistant, nosocomial outbreak pathogens remains a serious issue within healthcare. Genetic analysis of P. ursingii strains, clinical reports from closely related P. diazotrophicus and retrospective analysis of prior sepsis outbreaks suggest P. ursingii may represent a nosocomial, opportunistic pathogen with a propensity for ESBL antibacterial resistance. However, some organisms remain pan-sensitive, such as the bacteria isolated in the above case. This case is the first report of P. ursingii infection identified at the time of illness and hopes to serve as a basis to inform the clinician of antibacterial resistance risks, outbreak potential, clinical characteristics, treatment strategy and capacity for misclassification of P. ursingii. Our case’s main limitation remains the lack of a clear aetiology of Phytobacter infection. Further research is clearly needed to elucidate the clinical characteristics of this bacterium.
Learning points
Phytobacter ursingii is a newly described gram-negative organism that should be considered in patients with sepsis with recent use of parenteral nutrition or fluids; however, the organism has been isolated in sputum, pancreatic cysts, hospital wastewater, soil, urine, rectum and blood.
P. ursingii has been reported to have extended-spectrum antibacterial resistance so broad-spectrum antibiotics should be used until susceptibilities are elucidated for a given culture.
Phytobacter spp are commonly misidentified—even in modern laboratories. Databases such as the Matrix-Assisted Laser Desorption/Ionization Time of Flight helps more accurately identify this species, but care must be taken to ensure that Phytobacter spp are included in the reference database to prevent misidentifications.
Identification of Pantoea and Kluyvera spp on phenotypical or biochemical assays may warrant further biochemical testing as described in figure 3 to help prevent errant speciation of Phytobacter spp.
Ethics statements
Patient consent for publication
Footnotes
Contributors The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content—SC, KH, AS and EH. The following authors gave final approval of the manuscript—SC, KH, AS and EH.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.