Article Text

Abstract
A man in his 20s with a medical history of syphilis, chlamydia and HIV presented to the emergency department (ED) with 2 months of right hip pain and was found to have advanced avascular necrosis (AVN) of the right femoral head with secondary haemorrhage. The patient lacked the common risk factors of AVN in patients with HIV (PWH): ≥10 years of HIV diagnosis, extended duration on highly active antiretroviral therapy, trauma, corticosteroid use, alcohol abuse, systemic lupus erythematosus, obesity, smoking and dyslipidaemia. Given the extensive destructive changes in the hip joint and muscles, a right hip resection arthroplasty was performed, and the patient recovered well postoperatively. This case presents a learning opportunity for understanding bone pathologies in PWH and offers clinical guidance for the management of HIV-infected patients with a focus on optimising bone health.
- Orthopaedics
- HIV / AIDS
- Bone and joint infections
- Calcium and bone
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Background
The significance of this case lies in its potential to raise awareness regarding distinctive bone pathologies in individuals living with HIV and to elucidate optimal approaches to their medical management.
Case presentation
A man in his 20s with a medical history of syphilis, chlamydia and HIV presented to the emergency department (ED) with 2 months of right hip pain that had progressively worsened within the last month. Initially, 2 months ago, he sought outpatient care from a nurse practitioner when the pain started. After the negative lumbar X-rays (XRs), the pain initially was attributed to sciatica. There were no physical examination findings available from the initial visit. The pain continued to worsen after failing lidocaine patches and rest, eventually rendering the patient unable to ambulate. Two months later, a CT lumbar spine was ordered, which demonstrated right femoral head dislocation, erosive changes in the femoral head and acetabulum, as well as a large hip joint effusion. This prompted the patient’s visit to the ED the same day, where a physical examination revealed that the right lower extremity was shortened and externally rotated, consistent with the known deformity of the right hip. Sensation and vibratory sense were intact bilaterally as well as dorsalis pedis pulses. A hip examination performed in the ED revealed no active range of motion of the right hip. Passive range of motion to 45 degrees with flexion and abduction of the right hip was possible with pain past 45 degrees and pain with any internal rotation of the right hip. An MRI of the right hip was ordered, with findings raising concern for a superimposed septic arthritis and osteomyelitis.
This patient was incidentally diagnosed with HIV, chlamydia and syphilis during a general workup for health insurance 4 months prior to presentation. The patient stated that he completed treatment for chlamydia and syphilis and that he was compliant with his bictegravir/emtricitabine/tenofovir alafenamide regimen. The duration of his undiagnosed period is unknown. The patient reported no trauma, fever, recent infection, alcohol use, smoking or illicit drug use.
An infectious disease specialist was consulted, who recommended delaying antibiotics until the results of the surgical cultures were available. No arthrocentesis was performed preoperatively. Orthopaedic surgery was consulted, and a right hip resection arthroplasty procedure was performed. Intraoperatively, 30 mL of fluid from a right capsular haemarthrosis was obtained for cytology, soft tissue specimens from the hip were sent for culture, and bone debris from the acetabulum was sent to pathology. Three of each of the following cultures were collected from the right hip, including aerobic/anaerobic cultures, fungal cultures, and acid-fast cultures and smears. Cytological analysis of the right hip joint fluid revealed predominantly blood with the presence of lymphocytes, histiocytes and a few neutrophils, indicative of haemarthrosis. Subsequently, all cultures returned negative results, and the pathology report indicated ‘reactive and remodelling bone with associated bony destruction, consistent with advanced avascular necrosis’.
Investigations
On investigative workup, initial XR lumbar spine revealed no remarkable findings. Subsequent CT lumbar spine without contrast revealed right femoral head dislocation, total absorption of the femoral head and acetabulum, as well as a large hip joint effusion which prompted the patient to come to the ED. In the ED, XRs of the right femur and pelvis were ordered which demonstrated resorption of bone around the right acetabulum and proximal femur with a normal left proximal femur and acetabulum (figure 1). Preoperative MRI revealed lateral dislocation of the right femoral head, total absorption of the femoral head and high-grade tearing of the rectus femoris tendon and proximal adductor longus along with a haematoma in the right obturator externus (figure 2).

X-ray pelvis demonstrating resorption of the right femoral head and much of the femoral neck (taken at presentation during emergency department).

MRI right hip demonstrates lateral dislocation of the femoral head with complete resorption of the femoral head (yellow arrow) and thinning of the acetabular cortex (pink arrow). There is also tearing of the rectus femoris tendon (blue arrow) and proximal adductor longus (red arrow). Haematoma in the right obturator externus (green arrow).
Laboratory testing ordered on admission included, but was not limited to, white blood cell count (7.6×109/L, reference range: 4.0–12.0×103/µL), C-reactive protein (<1.0 mg/dL), erythrocyte sedimentation rate (92 mm/hour, reference range:0–15 mm/hour), urine drug screen (positive for cannabinoids), Neisseria gonorrhoeae DNA by urine PCR (negative), Chlamydia trachomatis DNA by urine PCR (negative), reflex rapid plasma reagin (reactive, 1:8), Quantiferon tuberculosis (negative), partial thromboplastin time (29.8 s, reference range: 23.0–35.0 s), prothrombin time (10.9 s, reference range: 9.0–13.0 s) and HIV-1 viral load (not detected). With the exception of a mild normocytic anaemia, which was likely secondary to HIV infection, all other laboratory findings were within normal limits. A lipid profile obtained 1 month prior to presentation was as follows: cholesterol 81 mg/dL (reference range: <200 mg/dL), triglycerides 59 mg/dL (reference range: <150 mg/dL), high-density lipoprotein 25 mg/dL (reference range: >40 mg/dL) and low-density lipoprotein 44 mg/dL (reference range: <100 mg/dL). At the time of HIV diagnosis 4 months ago, his viral load was 56 600 copies/mL, with a CD4 count of 346 cells/mm3. At the time of presentation, his viral load was undetectable, and his last known CD4 count of 518 cells/mm3, as of 3 months prior to presentation.
Differential diagnosis
Several differential diagnoses should be considered in this patient. The most likely differential diagnosis is avascular necrosis given the join pain, instability, altered gait, limited range of motion and the radiographic findings confirming the diagnosis. Next, infectious arthritis and osteomyelitis are plausible given the immunocompromised state associated with HIV and a sexually transmitted disease history. This is not supported by the lack of typical signs of an acute joint infection such as fever, severe pain, erythema and other systemic symptoms. Another possible diagnosis is traumatic avascular necrosis due to the high forces required for a hip dislocation as well as the haematoma. This is not supported by the absence of a clear traumatic event in the patient’s history. The least likely diagnosis would be HIV-associated polymyositis which is less likely as it presents with symmetric and proximal muscle weakness rather than the unilateral and unifocal involvement observed in this case.
Treatment
Treatment involved right hip resection arthroplasty. During surgery, it was noted that the femoral head had completely collapsed, with severe erosive changes and complete destruction of most of the acetabular labrum. Postoperative pain management consisted of acetaminophen and ibuprofen as needed. No other new medications were prescribed.
Outcome and follow-up
After the right hip resection arthroplasty, inpatient physical therapy began and continued with outpatient sessions. He was discharged home and was advised to remain non-weight bearing for 4 weeks postoperatively and use a wheeled walker to ambulate. The patient experienced no postoperative complications and reported no pain. All follow-up laboratory findings were within normal limits. Once the patient is medically stable and recovered, there are plans for a right hip conversion to a total right hip arthroplasty.
Discussion
HIV has been a major public health problem since its emergence in the 1980s, and as of 2019, there are 3.69 million HIV/AIDS cases worldwide.1 Despite advances in HAART, HIV remains a major contributor to morbidity and mortality worldwide. As an inflammatory multisystem disease, HIV acts through a multitude of mechanisms and causes a wide range of pathology. Mechanisms include, but are not limited to, release of inflammatory cytokines such as interleurkin-6 (IL-6), interleukin-10 (IL-10), interleukin-15 (IL-15), tumour necrosis factor and elevated monocyte turnover/activation resulting in accelerated atherosclerosis.2 PWH are at increased risk of diabetes (OR 1.45), hypertension (OR 1.36), stroke (OR 1.45), cancer (OR 1.37), lung disease (OR 1.33), and numerous other chronic and acute illnesses.3 Of particular interest in this article, PWH are significantly more likely to experience bone-related pathologies such as fractures, osteoporosis, osteonecrosis compared with the general population. Patients with HIV are twice as likely to have a history of fracture, 3.7 times as likely to develop osteoporosis and 100 times more likely to develop osteonecrosis.4–6 The mechanism of bone disease in patients with HIV has not been fully elucidated. The chronic inflammatory processes associated with HIV are thought to stimulate receptor activator of nuclear factor kappa beta (RANKL) production and increase bone resorption. In vitro studies have also shown HIV proteins Tat and Nef induce senescence of bone marrow mesenchymal cells, thus preventing osteoblast formation through nuclear factor-kappa B activation.7 In individuals with HIV infection, there is evidence of B cell dysregulation characterised by elevated B cells expressing RANKL and a reduced population of B cells expressing osteoprotegerin (OPG).8 Treatment options for patients with HIV, specifically highly active antiretroviral therapy (HAART), have significantly reduced mortality and morbidity among PWH and have improved the quality of life for millions of patients worldwide.9 Unfortunately, with regard to bone health, the initiation of HAART causes a loss of 2–6% of bone mineral density (BMD) over the first 96 weeks of therapy and as demonstrated by the Strategies for Management of Antiretroviral Therapy (SMART) trial, bone loss with the introduction of HAART is greater than bone loss caused by HIV alone.10 11 The mechanism of this loss is not known but medications such as efavirenz and protease inhibitors are known to inhibit the action of 25-hydroxylase and 1-alpha-hydroxylase.12 The resulting vitamin D and OPG/RANK/RANKL dysregulation combined with increased bone turnover by stimulated osteoclast differentiation and activity are possible explanations for the negative impacts on BMD. HAART regimen should be initiated considering varying medication effects on BMD. Three nucleoside reverse transcriptase inhibitors (NRTIs)—zidovudine-lamivudine combination, lamivudine-abacavir combination, and abacavir—and three protease inhibitors (PIs)—lopinavir-ritonavir combination, ritonavir and atazanavir—were associated with an increased risk of osteoporosis.13
In analysing which PWH are at higher risk of bone pathology, Lima et al conducted a retrospective analysis of 44 PWH with stage 3 and 4 osteonecrosis of the femoral head. The most common presentation was bilateral hip necrosis (70.5%). They found that the average patient had been living with HIV for 12 years, had a CD4 lymphocyte count of ~525 cells/mm3 and had been on HAART for 10 years. Of patients on HAART, 100% had used NRTIs, 83% had used non-nucleoside reverse transcriptase inhibitor (NNRTI) and 66.7% had used PIs. In addition, dyslipidaemia was found in 48% of patients, history of alcoholism in 50% and smoking (previous or current) in 77.2%.14 Another study by Borges et al found that white race, prior osteonecrosis, prior fractures, history of AIDS-defining conditions, prior exposure to didanosine, indinavir, saquinavir, ritonavir boosted lopinavir, or tenofovir-disoproxil-fumarate and lower CD4 counts are associated with increased risk of osteonecrosis.15
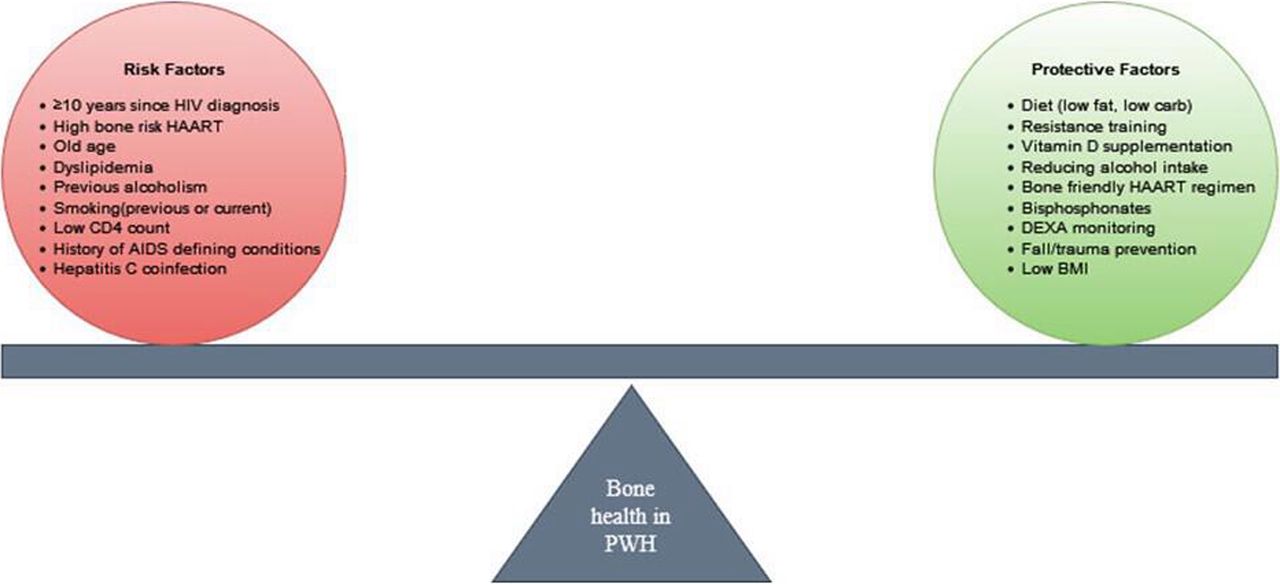
While PWH are inevitably at higher risk of pathologies such as osteopenia, osteoporosis, osteomalacia due to calcium and bone dysregulation that accompanies HIV, clinical management of PWH should consider impacts on bone health (figure 3). While the risk-return assessment obviously favours HAART, clinicians dealing with PWH should evaluate risk factors for bone pathology and guide treatment accordingly to minimise the impact of HIV and its treatment. Several strategies can be used to accomplish this task. Clinicians should encourage patients to maintain a diet that prevents dyslipidaemias, one of the risk factors for osteonecrosis. Restricting simple carbohydrates and added sugars which are known to increase triglycerides and increasing the amount of fibre and plant sterols/stanols are specific goals that can be targeted when optimising diet for PWH.16 In addition, pharmacological interventions such as statins and fibrates should be used as indicated. Resistance training should also be incorporated as mechanical load is known to stimulate the osteogenic effects for increasing bone mass.17 Vitamin D level reduction is common during HIV disease progression and is linked to decreased survival rates and supplementation has been shown to increase BMD, decrease inflammation and increase CD4 T cell count. Supplementation with 4000 international units (IU) of vitamin D is recommended.18 Use of bisphosphonate drugs in PWH has been shown to have a comparable impact in increasing BMD to the general population. There is evidence for the prophylactic use of bisphosphonates as a clinical trial demonstrated that a single 5 mg dose of zolendronic acid on HAART initiation decreases bone resorption and BMD loss in untreated PWH for 3 years.19 Finally, tailoring HAART regimens to be bone friendly by avoiding the use of certain NRTIs, NNRTIs and PIs in patients with a greater number of risk factors.

{kind=link}
{kind=link}
{kind=link}
Maintaining optimal bone health in patients with HIV (PWH) (author: SR). BMI, body mass index; HAART, highly active antiretroviral therapy.
The presented case aligns with the established understanding that PWH face an elevated risk of various bone-related pathologies, such as fractures, osteoporosis and osteonecrosis. Although this patient exhibited unilateral avascular necrosis of the right hip and a history of HAART, the absence of typical risk factors provides a valuable learning opportunity. The patient’s young age, lack of previous bone-related pathology, brief duration of HAART use, no history of corticosteroid or alcohol use, and the unilateral presentation present a scenario where conventional risk factors do not align. This emphasises the need to reconsider potential unique contributors to AVN in PWH.
Furthermore, the patient exhibited extensive injuries to surrounding tendons and along with a haematoma in the right obturator externus. One plausible explanation is that these injuries and haematomas resulted from the mechanical changes induced by the collapse of the femoral head. The altered biomechanics and heightened stress on surrounding soft tissues, stemming from the patient’s attempt to ambulate for several months before seeking medical attention, likely contributed to microtrauma and strain on the muscles.
Learning points
Healthcare providers should be vigilant about bone health in patients with HIV (PWH), given the increased risk of bone-related pathologies. Patients may present with atypical clinical signs, and providers should be aware.
Management of PWH should be conducted with a comprehensive approach involving diet, vitamin D supplementation and judicious selection of highly active antiretroviral therapy to mitigate bone loss.
For PWH presenting with musculoskeletal complaints, timely consultations with infectious disease specialists, orthopaedic experts and other relevant healthcare professionals are essential to effectively rule out concurrent infections or septic arthritis.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content: SR, NK. The following authors gave final approval of the manuscript: NK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.