Article Text

Abstract
Small bowel obstruction (SBO) is a leading cause of general surgery inpatient admissions. SBO is most commonly associated with postoperative adhesions; however, neoplastic SBO is an important differential. Here, we present a case of neoplastic SBO secondary to leiomyosarcoma in a patient with known mature B cell lymphoma. This case highlights the importance of avoiding early diagnostic closure and adherence to oncological principles of resection for small bowel tumours.
- Small intestine cancer
- General surgery
- Surgical oncology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Background
Small bowel obstruction (SBO) is a common general surgical pathology, responsible for up to 15% of inpatient general surgery admissions in North America annually.1 SBO is most commonly associated with adhesions related to prior abdominal and/or pelvic surgery (75%).2 Less common causes include abdominal wall hernias, Crohn’s disease and small bowel (SB) neoplasia (5%).2
Neoplastic SBO can be caused by a variety of disease processes. These processes range from primary SB malignancies such as adenocarcinoma, leiomyosarcoma or neuroendocrine tumours (NET) to metastatic lesions involving the SB, mesentery or peritoneum. Primary lymphoma may develop in the SB; however, more frequently, the SB or mesenteric lymph nodes are involved secondarily in a systemic lymphoma. Collectively, lymphoma is one of the most common neoplastic processes involving the SB prompting emergency presentation.3 4 By contrast, sarcoma involving the SB is exceedingly rare, accounting for only 10% of SB neoplasms.5 Gastrointestinal stromal tumours are the most common form of SB sarcoma (86%), followed by leiomyosarcomas (3%).6 Irrespective of the underlying cause of SB neoplasia, only 22% of patients present with SBO.7 Unlike adhesional SBO that typically resolves without operative intervention,8 neoplastic SBO often requires surgical intervention.9
Here, we present a rare case of SBO due to primary SB leiomyosarcoma in a patient with known lymphoma.
Case presentation
A man in his 80s was diagnosed with SBO following a presentation to the emergency department with colicky abdominal pain, obstipation, nausea and vomiting. His vital signs were unremarkable, and his abdomen was distended but non-tender.
The patient’s background was significant for lymphoplasmacytic lymphoma, a low-grade mature B cell lymphoma, on active surveillance after a recent episode of febrile neutropenia while on zanubrutinib, during which an incidental, non-obstructing SB mass was identified. Further history included rheumatoid arthritis and collagenous colitis managed with oral sulfasalazine 1.5 g two times per day and 6 mg of prednisolone daily. He previously had an open appendicectomy.
Investigations
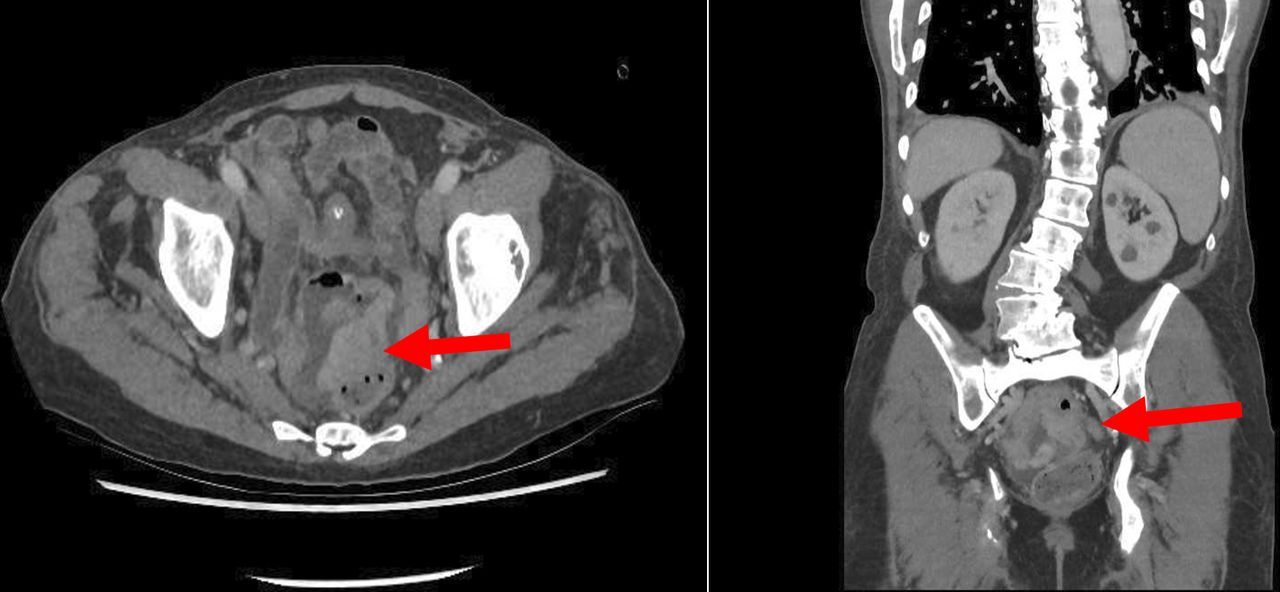
Blood tests revealed a normocytic, normochromic anaemia with a haemoglobin level of 101 g/L. Inflammatory markers included a white cell count of 11.9×109 cells/L and C reactive protein of 71 mg/L. Electrolytes, renal and liver function test results were unremarkable. CT of his abdomen-pelvis with portal venous contrast demonstrated a large obstructing distal SB mass (figure 1), which increased in size compared with a CT performed during his admission for febrile neutropenia 4 months prior (figure 2).

Single slice axial (left) and coronal (right) CT images at time of presentation with small bowel obstruction demonstrating a soft tissue mass (red arrow) involving loops of small bowel in the pelvis.

{kind=link}
{kind=link}
Single slice axial (left) and coronal (right) CT images demonstrating soft tissue mass (red arrow) at time of identification.
Treatment
Initial management involved nasogastric tube decompression and intravenous fluid resuscitation. Gastrografin was administered on the second day of admission with clinical and radiological resolution of the obstruction. The initial impression was that the mass was likely a SB lymphoma that progressed following the cessation of zanubrutinib. Haematology was consulted, and it was advised that lymphoplasmacytic lymphoma less frequently involves the SB and is unlikely to be related to the SB mass. Given this advice and the progression of the now symptomatic SB mass over time, the decision was made to proceed with surgical resection.
Laparoscopy demonstrated an SB mass adherent within the pelvis. Adhesiolysis was performed through a lower midline laparotomy to allow an oncological, stapled, side-to-side, antiperistaltic SB resection. The SB lumen was significantly narrowed by the mass, and multiple enlarged, firm mesenteric lymph nodes were palpable. There was no evidence of metastatic disease.
Outcome and follow-up
The patient progressed well and was discharged from the hospital on postoperative day 7.
Histopathology demonstrated a 75 mm grade 2 jejunal leiomyosarcoma with negative margins and one of four lymph nodes demonstrating metastatic disease. The remaining three lymph nodes showed features consistent with known lymphoplasmacytic lymphoma. Epstein-Barr virus (EBV)-encoded RNA was negative, and the possibility of an EBV-associated leiomyosarcoma was excluded. Staging CT chest was negative. The case was discussed in a multidisciplinary meeting that concluded only ongoing surveillance was required.
Discussion
This case demonstrates the importance of maintaining a broad differential diagnosis and considering multidisciplinary discussion for patients with potentially neoplastic SBO.
Patients with lymphoma do rarely present with concurrent sarcoma, most commonly histiocytomas, angiosarcomas and radiation-associated soft tissue sarcomas.10 Patients with EBV may present with Hodgkin lymphoma (HL) and very rarely leiomyosarcomas;11 however, to date, there are no reported cases in the literature of concurrent SB leiomyosarcoma in patients with mature B cell lymphoma causing an obstruction.
While the gastrointestinal system is the most common site of extra-nodal disease in lymphoma, not all subtypes are likely to present in this fashion. Secondary extra-nodal involvement is more likely to occur in non-Hodgkin's lymphoma (NHL) than in HL. Indolent lymphomas are less likely to have extra-nodal disease compared with aggressive forms of NHL. Of the histological subtypes, diffuse large cell B cell lymphoma (DLBCL), particularly high-grade DLBCL, is most frequently associated with extra-nodal disease.12 Mantle cell lymphoma, Burkitt and Burkitt-like lymphomas have also been shown to frequently involve the SB.13 14 The patient presented above was diagnosed with lymphoplasmacytic lymphoma, an indolent B cell NHL that typically involves lymph nodes, bone marrow and the spleen. Although involvement of the stomach and bowel has been reported,15 16 in general, extra-nodal involvement in lymphoplasmacytic lymphoma is rare.17
While specific therapies are tailored to the subtype, systemic treatments are first line for both HL and NHL.18 In the absence of indications for urgent surgery, such as perforation and haemorrhage, a period of observation to assess for response to systemic therapies is attempted before proceeding to resection of any symptomatic extra-nodal disease.
In contrast, non-lymphoma SB malignancies (adenocarcinoma, sarcoma and NET) are managed with oncological resection where possible. For adenocarcinoma, a segmental resection with a margin of normal SB and mesentery is important for adequate nodal resection and staging.19 Similarly, for SB NET, a wide en-bloc resection including mesentery and lymph nodes is recommended due to the high risk of nodal metastasis.20 R0 resection margins are crucial for the management of any sarcoma to reduce the risk of local recurrence.21 22 Unlike adenocarcinoma and NET, nodal metastases in sarcoma are rare,23 and in biopsy-proven cases, routine lymphadenectomy may not be required.
These differences in management further reinforce the need for careful diagnostic consideration and multidisciplinary discussions for patients presenting with potential neoplastic SBO. If surgery is required, despite what the suspected underlying pathology may be, oncological principles are recommended to ensure negative resection margins and adequate sampling of mesenteric nodes for prognostication.
Learning points
Although the gastrointestinal system is the most common site of extra-nodal involvement in lymphoma, some lymphomas are more likely to involve the small bowel (SB) than others.
Potential neoplastic SB obstruction requires a broad differential, and, even in patients with known malignancy, second primaries are possible; a multidisciplinary discussion is helpful when considering operative management.
Always adhere to oncological resection principles where possible. For sarcoma, a negative resection margin without spillage is essential, while for neuroendocrine tumours and adenocarcinoma, adequate nodal sampling is also required for accurate staging and prognostication.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content: AS. AS was the primary author for drafting, sourcing and editing of images and results. SSD and KN provided critical revisions and edits to the drafts. The following authors gave final approval of the manuscript: AS, SSD and KN. Guarantor: KN.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.