Article Text

Abstract
Immune checkpoint inhibitors (ICIs) block inhibitory pathways that tumour cells exploit to evade the immune system. They play a key role in the management of aggressive cancers, including non-small cell lung cancer, melanoma and Hodgkin’s lymphoma. Despite their efficacy, ICIs can cause severe, potentially fatal, immune-related adverse events (irAEs), including multiorgan failure. We present a case of a woman in her early 70s with metastatic lung adenocarcinoma recently initiated on pembrolizumab who presented with an acute stroke complicated by irAE-related multiorgan failure. Despite aggressive treatment, the patient remained critically ill and passed away the same day after transitioning to end-of-life care. This case emphasises the life-threatening potential of irAEs, the importance of early diagnosis and the challenges of managing these complications. Clinicians should maintain a high index of suspicion for irAEs in ICI-treated patients to optimise timely intervention and outcomes.
- Cancer intervention
- Immune Checkpoint Inhibitors
- Malignant disease and immunosuppression
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The management of malignancy is multimodal, often comprising some combination of surgery, chemotherapy and radiation therapy. However, in the last few decades, immunotherapy has advanced the treatment of many malignancies, including many aggressive cancers such as non-small cell lung cancer, melanoma and Hodgkin’s lymphoma.1 These treatments target key receptors in the immune system, including cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein-1 (PD-1), which function as immune checkpoints and are negative regulators of T-cell immune function.2 CTLA-4 can potently upregulate lymphocyte function-associated antigen 1 (LFA-1) adhesion using receptor clustering.3 Active LFA-1 is needed for antigen presentation by antigen-presenting cells and migration of T-cells to intravascular regions, peripheral lymph nodes and inflammatory sites. However, cancer cells have evolved mechanisms against these immune checkpoints to downregulate T-cell activation and evade immune detection.4
Immune checkpoint inhibitors (ICIs) inhibit these negative regulatory components of the immune response targeted by tumour cells, like CTLA-4 and PD-1, leading to enhanced T-cell action against cancer cells.5 One specific agent, pembrolizumab, is a monoclonal antibody that binds to the PD-1 receptor on T-cells, impeding the interaction between the PD-1 receptor and its ligands (PD-L1 and PD-L2) expressed on tumour cells.1 Inhibiting the interaction between PD-1 and PD-L1 allows for T-cell activation, proliferation and cytotoxic secretion to produce antitumour immune responses.6
Enhancing the immune system can, however, lead to a unique constellation of inflammatory toxicities that may warrant discontinuation of therapy and/or administration of immunosuppressive agents.7 The broad activation can initiate unwanted autoimmune inflammation in patients, including a wide spectrum of vital organs such as the pituitary gland, thyroid gland, lungs, liver and kidneys.8 Infrequently, these adverse effects of ICIs can even present as severe complications, such as organ failure, which can ultimately be fatal, and are collectively termed immune-related adverse events (irAEs).9 The onset of most irAEs is usually delayed, within weeks to months of initiation, however, a hyperacute presentation is extremely rare, particularly with multiorgan involvement. 9 We present an unfortunate case of a rapid multiorgan failure requiring intensive care unit (ICU) admission in a patient in her early 70s with metastatic recurrence of lung adenocarcinoma 1 week after pembrolizumab initiation.
Case presentation
A woman in her early 70s with metastatic lung adenocarcinoma status post left lung resection initiated on adjuvant treatment with pembrolizumab 1 week prior to admission was brought in by ambulance for altered mental status with concerns for stroke. Initial presentation at the emergency department was notable for severe hypotension, with a blood pressure of 80/60 mm Hg on admission, hypoglycaemia with a glucose level in the low 40s (mg/dL) and aNational Institute of Health Stroke Scale (NIHSS) score of 22. Physical examination revealed altered mental status, an anisocoric right pupil with an absent pupillary light reflex and left-sided motor deficits, without evidence of fever, rash or joint pain. CT angiography (CTA) of the head demonstrated an acute occlusion versus severe stenosis of the right middle cerebral artery (MCA) inferior M2 distal branch. Pertinent laboratory findings on admission included pancytopenia (white blood cell count of 1.0×10⁹/L with neutrophil count of 0.6×10⁹/L and eosinophil count of 0, haemoglobin of 9.4 g/dL (baseline 14 g/dL), platelets of 76×10⁹/L), hyponatraemia (123 mmol/L), hypokalaemia (2.4 mmol/L), stage III acute kidney injury (creatinine 2.27 mg/dL; baseline 0.7 mg/dL), severely elevated transaminases (Aspartate aminotransferase (AST) >7000 U/L, alanine aminotransferase (ALT) 3839 U/L, prothrombin time (PT) 24.2 s, international normalized ratio (INR) 2.09) and severe lactic acidosis (lactate 11.4 mmol/L). C-reactive protein (CRP) was not obtained.
The patient was transferred to the ICU for undifferentiated shock requiring pressors complicated by severe acute renal and liver failure. CT of the abdomen/pelvis on admission demonstrated oesophagitis, pancolitis, bilateral renal infarcts and cholangitis (figures 1–3). The primary team reached out to the patient’s primary oncologist. The patient received cycle 1 day 1 (C1D1) paclitaxel, carboplatin and pembrolizumab a week before current presentation, with the patient’s labs and imaging prior to initiation within normal limits. The patient’s primary oncologist expressed concern for potential adverse reaction from pembrolizumab, and thus the inpatient oncology team recommended initiating high-dose steroids with intravenous methylprednisolone 2 mg/kg/day. In addition to the high-dose steroids, the patient received significant volume resuscitation and was started on broad-spectrum antibiotics (piperacillin-tazobactam) and vasopressors. However, the patient remained critically ill in multiorgan failure. After discussion with the family, the patient was transitioned to end-of-life care and expired less than 12 hours after presentation.

Axial view of oesophagitis seen on CT of the abdomen/pelvis with contrast. Yellow arrow points to the inflamed oesophagus.

Coronal view of pancolitis as seen on CT of the abdomen/pelvis with contrast. Green arrows point to several areas of inflamed bowel.

Coronal view demonstrating bilateral renal infarcts seen on CT of the abdomen/pelvis with contrast. Orange arrows point to areas of infarct.
Investigations
No other investigations other than those listed previously were obtained given the rapid decline of the patient’s status.
Differential diagnosis
On discussion with the patient’s primary oncologist, it was found that the patient’s CT of the abdomen/pelvis a week before admission from an outside facility was without any acute findings. Images were not available at the time of admission to compare with and neither were lab values. Current imaging findings were thought to be secondary to irAEs.
The differential diagnoses were broad, including sepsis as an aetiology for multiorgan failure. However, blood cultures remained negative and there was low suspicion for an infectious aetiology as there was no obvious source seen on imaging or on physical exam. Even though the patient originally presented with concerns for an acute stroke as the main aetiology for encephalopathy, the differential was confounded by the simultaneous liver failure and renal failure. CT of the head without contrast did not demonstrating significant structural concerns such as haemorrhage or encephalitis and CTA of the head did demonstrate severe stenosis versus an occlusion of the distal branch of the right MCA. However, due to the patient’s rapid decline, it was not possible to obtain MRI to evaluate the degree of stroke.
Treatment
The patient was volume-resuscitated and was started on Zosyn, high-dose intravenous steroids and vasopressors for hypotension. However, the patient remained critically ill in multiorgan failure.
Outcome and follow-up
After discussion with the family, who endorsed the patient would not want to continue life-sustaining treatments such as intubation if the outcomes appeared poor, and with persistently high pressor requirements, the patient was transitioned to end-of-life care and expired later that same day.
Discussion
The literature on the rapid emergence of irAEs is limited, with the average onset varying depending on the specific irAE.9 However, prior case reports have documented severe irAEs similar to our patient’s presentation. A PubMed literature search using the keywords ‘multi-organ failure’, ‘immunotherapy’, ‘immune checkpoint inhibitors (ICI)’, ‘irAE’ and ‘cancer’ identified six relevant case reports meeting our inclusion criteria of keywords, ICI therapy and rapid onset of symptoms (defined as within 1 month of treatment). Among these case reports, the earliest reported onset of irAEs occurred at 2 weeks.10 11 Brazel et al10 described a case of rapid multiorgan failure 14 days after a single dose of combination therapy with nivolumab and ipilimumab for metastatic melanoma. The patient developed renal failure, drug-induced hepatitis and myocarditis.10 Similarly, Xie et al11 reported a case of multiorgan failure involving fulminant myocarditis, myasthenia gravis crisis and hepatic dysfunction occurring 14 days after the initial pembrolizumab dose for large cell neuroendocrine carcinoma. The patient experienced symptom improvement with pacemaker placement and high-dose steroids and was discharged 43 days after hospitalisation.11 However, the patient was readmitted 2 weeks later with presumed delayed immune-related pneumonitis, which resolved completely with steroid and antibiotic therapy.11 Other case reports highlight severe ICI-related complications, with some demonstrating symptom improvement following steroids and targeted treatments. However, to our knowledge, no published case reports have documented a rapid onset of multiorgan failure within 1 week of a single dose of pembrolizumab, as observed in our case.
The adverse effects of ICIs are well documented, varying in clinical presentation and timing. However, it is exceedingly rare to observe multiple concurrent organ involvement, as exemplified by our patient’s case of multiorgan failure. irAEs are classified into five classes, with grades 1–2 being mild to moderate, grade 3 indicating severe, grade 4 signifying life-threatening complications and grade 5 pertaining to events resulting in death secondary to toxicity12 (table 1). The mechanism of irAEs is not well elucidated, but the proposed mechanisms involve an intricate interplay of pathways involving autoreactive T-cells, autoantibodies and elevated inflammatory cytokines.13
A summarised list of some immune-related adverse events based on toxicity, guidance to discontinue immune checkpoint inhibitor (ICI) and whether steroid can be used or not
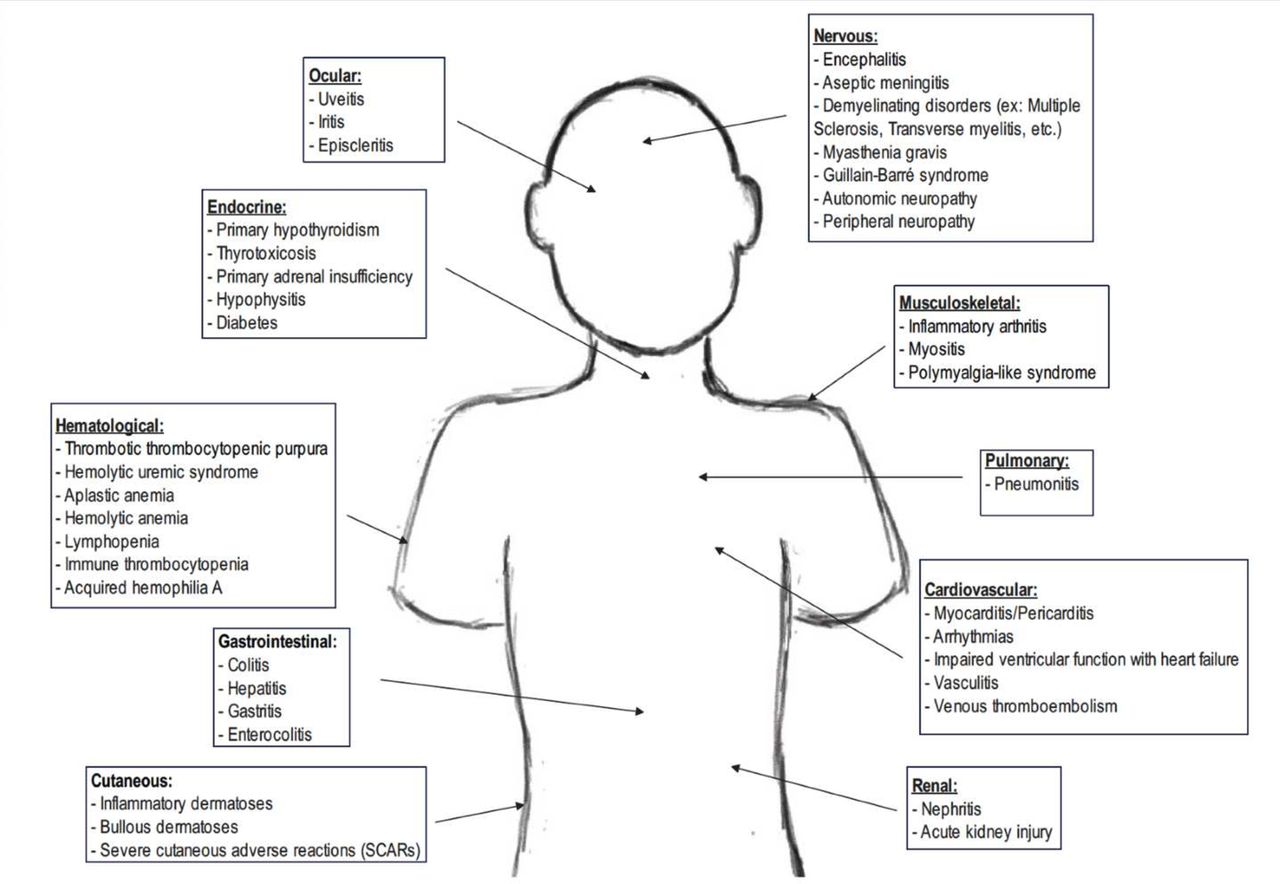
Our patient’s clinical presentation is especially noteworthy given the emergence of numerous grade 3–4 irAEs, especially within a short span of initiation of pembrolizumab for metastatic lung adenocarcinoma. Retrospective studies have demonstrated that colitis, hepatitis, adrenocorticotropic hormone insufficiency, hypothyroidism, acute kidney injury and myocarditis were some of the most common adverse inflammation reactions seen secondary to ICIs14 ().

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graphical representation of adverse inflammatory reactions secondary to immune checkpoint inhibitors. This image was drawn by the authors.
Although the presentation and severity of these irAEs varied, they can also be self-limited and treated with steroids, with resumption of immunotherapy when the patient recovers from the initial event.8 Given our patient’s rapid demise, further workup was not able to be done to see if they had other irAEs that may have developed with time. It is unclear what factors led our patient to a rapid decline; however, it can be speculated that age, comorbid conditions and other underlying adverse effects contributed to the presentation.
Depending on grade, treatment ranges from conservative management with continuation of immunotherapy versus discontinuation of therapy with corticosteroid initiation and sometimes further immunosuppression in refractory cases.15 Standard of care involves ruling out alternative causes of organ dysfunction; however, rapid decline may occur, necessitating early administration of steroids, while alternate causes are not ruled out. Corticosteroids are usually tapered off in 4–6 weeks; however, no specific guidelines are available on intravenous versus oral steroids.15 The European Society for Medical Oncology (ESMO) also has guidelines on the incidence and management of irAEs as seen with the American Society of Clinical Oncology (ASCO) guidelines.16 In comparison, the guidelines presented by ESMO are similar to ASCO, with an algorithmic framework and extensive workup discussion for ruling out alternative diagnoses, as well as steps to management. ASCO and ESMO similarly recommend in most cases use of corticosteroids for grade 3 or higher irAEs, with distinct regimens presented per the irAE and with clear guidelines on discontinuation versus reinitiation.16 ESMO guidelines for managing irAEs align with ASCO’s guidelines in severity classification of irAEs and depending on the severity, using corticosteroids as first-line treatment with gradual tapering, but highlights the use of biologics like infliximab and mycophenolate in refractory cases more explicitly than ASCO.16
Diagnosing irAEs can be challenging and necessitates a high index of suspicion as they can manifest as severe complications, including organ failure and in some cases death. While infrequent, a comprehensive understanding of the nature of irAEs is vital to the diagnosis and management of such life-threatening toxicities. Physicians should have a high suspicion for adverse effects due to immunotherapy regardless of timeline of initiation.15
Learning points
All medical professionals involved in the care of a patient on immunotherapy should have a high suspicion for immune-related adverse events (irAEs).
Prompt treatment with removal of the offending agent and possibly steroids should be initiated.
The timing of immunotherapy can vary with the onset of adverse events and therefore irAEs should always be on the differential.
Ethics statements
Patient consent for publication
Footnotes
Contributors The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content: TV, AJ, SA. The following authors gave final approval of the manuscript: TV, AJ, SA. Guarantor: TV.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.