Article Text

Abstract
A well-managed hypertensive and dyslipidaemic female in her 60s presented with a 4 month history of progressive visual decline, ocular irritation and localised erythema in her right eye. These ocular symptoms were associated with repeated exposure to environmental water sources. Clinical evaluation revealed marked conjunctival injection, corneal oedema, diffuse stromal haze and a dense infiltrate with a 6×6 mm epithelial defect at the central cornea. A penetrating keratoplasty revealed acid-fast bacilli in the corneal pathology, confirmed as Mycobacterium haemophilum via the line probe assay. Mycobacterial growth was absent in culture.
A comprehensive treatment regimen, including systemic amikacin, levofloxacin, rifampicin, azithromycin and topical antituberculous therapy, resulted in significant clinical improvement. This case highlights M. haemophilum as an infrequent cause of non-tuberculous mycobacterial keratitis. Recurrent eye contact with contaminated water was shown as a notable risk factor in the absence of prior corneal interventions.
- Infectious diseases
- TB and other respiratory infections
- Anterior chamber
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Non-tuberculous mycobacteria (NTM) are a group of atypical mycobacteria characterised by their aerobic, non-motile and non-spore-forming nature.1 These pathogens are typically found in reservoirs such as soil, dust and water.2–4 Human infections typically arise from environmental exposures.3 4
NTM infections typically have a sluggish disease course, making prompt identification difficult. Consequently, there is often a substantial delay in diagnosis or initial misdiagnosis, resulting in delayed treatment initiation and increased morbidity.4
While ophthalmic infections resulting from opportunistic pathogens are infrequent, their prevalence and diversity have witnessed an upward trajectory in recent decades.4 The majority of reported cases of NTM ophthalmic infections involved keratitis, followed by endophthalmitis, cutaneous periocular infection, scleritis, dacryocystitis and canaliculitis, orbital infection, uveitis and conjunctivitis.3 4 Ophthalmic infections are primarily associated with rapidly growing mycobacteria; however, infections caused by slowly growing mycobacteria, though rarer, have also been documented in human eyes through case reports.3–5
Although keratitis stands out as the most prevalent form of ocular NTM infection, it is frequently preceded by ocular interventions. Laser-Assisted In Situ Keratomileusis (LASIK) emerges as the most common procedure, followed by cataract surgery, keratoplasty and excision of pterygium/pinguecula, identified as prominent risk factors.4
Mycobacterium haemophilum belongs to the slow-growing subgroup known as non-photochromogens. This organism is abundantly present in the environment and is primarily found in water sources.6 7 Infections caused by the pathogen predominantly affect immunocompromised populations, manifesting in various clinical presentations.8
According to the literature and to the best of our knowledge, keratitis caused by M. haemophilum is quite rare. Only three reports of M. haemophilum keratitis have been previously published.5 9 10 We present a unique case of M. haemophilum infection in a cornea without prior surgical intervention, posing challenges with both diagnosis and treatment.
Case presentation
A woman in her 60s, with a medical history of well-managed hypertension and dyslipidaemia, presented with a gradual decline in vision, ocular discomfort and localised erythema with minimal yellowish discharge in her right eye over a 4 month period. She denied experiencing fever, weight loss or respiratory issues. There was no history of tuberculosis contact. She did disclose recurrent contact with environmental water sources in the 2 months leading up to the onset of symptoms. Rainwater stored in a natural well had become contaminated with soil and fallen leaves. She reported using it for facial cleansing during her vacation rental trip. One month after the initial symptoms appeared, she underwent empirical treatment for herpes keratitis with valacyclovir and topical methylprednisolone.
The patient’s symptoms continued to persist, and her vision deteriorated to 2 m. She also reported noticing a white spot on her cornea, which showed signs of progression. Despite undergoing multiple courses of over-the-counter antibiotics and antihistamine eyedrops during the following months, the ocular complaints persisted with increased pain and discomfort. Additionally, the white spot on her cornea progressed to encompass her entire right cornea. As a result, vision in her right eye was reduced to perceiving only motion and light nearby. She retained functional abilities such as walking, writing and performing activities using her single left eye.
A year earlier, the patient had been diagnosed with suspected Herpes Simplex Virus (HSV) keratitis and recurrent anterior uveitis in the right eye. She had undergone a brief regimen of systemic and topical steroids lasting 6 weeks. While her vision exhibited improvement, a minor corneal scar persisted. Her initial visual acuity in the right eye after treatment for suspected HSV keratitis and recurrent anterior uveitis and preceding this episode was 20/32 with a pinhole correction of 20/20.
On examination of the right eye, severe impairment of visual acuity limited to hand motion with poor projection of light was noted. Clinical assessment established marked conjunctival injection, corneal oedema and the presence of a diffuse stromal haze. A dense infiltrate with an epithelial defect measuring 6×6 mm was identified in the prominently posterior stroma at the central area of the right cornea, accompanied by a 2 mm hypopyon in the anterior chamber (figure 1A). The respiratory and cardiovascular systems displayed no notable abnormalities, and there were no signs of hepatosplenomegaly or lymphadenopathy.

Right eye examination (with the patient’s permission) revealed significant conjunctival injection and central corneal infiltration with diffuse stromal haze at admission (A) and progression of the dense infiltration before therapeutic penetrating keratoplasty (B).
Investigations
The confocal scan of the cornea did not reveal the presence of acanthamoeba cysts or fungal hyphae. Ocular ultrasonography revealed scleral and choroidal thickening, accompanied by fluid accumulation in Tenon’s capsule, with no evidence of vitritis.
The initial corneal scraping was subjected to fresh smear examination, along with Gram staining, Kinyoun staining, potassium hydroxide staining and modified trichrome staining, all of which revealed no evidence of organisms. Furthermore, conventional aerobic bacterial, mycobacterial and fungal culture methods showed no growth of any causative pathogen.
Additionally, anterior chamber tapping for Gram staining and aerobic bacterial culture, alongside molecular studies targeting the herpes virus, yielded negative results. Blood cultures set for aerobic and anaerobic bacteria to exclude endogenous endophthalmitis were negative.
Testing for anti-HIV antibodies and interferon gamma autoantibodies also returned negative results, and glycosylated haemoglobin measured at 5.8 mg%. Optical coherence tomography was not feasible since the patient could only perceive hand motion and was unable to maintain eye fixation. Additionally, the high opacity of the anterior chamber was anticipated to result in a low yield from the examination.
Despite diligent efforts with empirical treatment, involving a combination of antibiotics (cefazolin and ceftazidime eyedrops), antifungals (systemic voriconazole and eyedrops) and antivirals (systemic acyclovir), the corneal lesion continued its progressive deterioration (figure 1B).
Differential diagnosis
Given the chronic and progressively worsening of the symptoms, lack of response to multiple courses of systemic and topical antimicrobial treatments, and a tendency for low-virulence pathogens, the focus shifted towards NTM and fungal origins rather than acanthamoeba, herpes or bacterial causes. The patient’s history of recurrent exposure to environmental factors and steroid use further increased the likelihood of these pathogens.
The initial negative outcome from corneal scraping might be attributed to potential pathogen infiltration into deeper corneal layers. Given the persistent infection, more invasive approaches such as corneal surgery may be warranted to procure microbiological evidence and gain control over the infection.
Furthermore, molecular studies assume critical importance, particularly when staining and culture results are negative, potentially due to prior exposure to antibiotics and antifungals.
Treatment
Therapeutic penetrating keratoplasty was selected as the intervention strategy, using a temporary glycerine-preserved corneal graft due to the current shortage of fresh donor tissue. This approach aimed to control the infection, obtain microbiological evidence, and plan for a definitive corneal graft once the infection was under control.
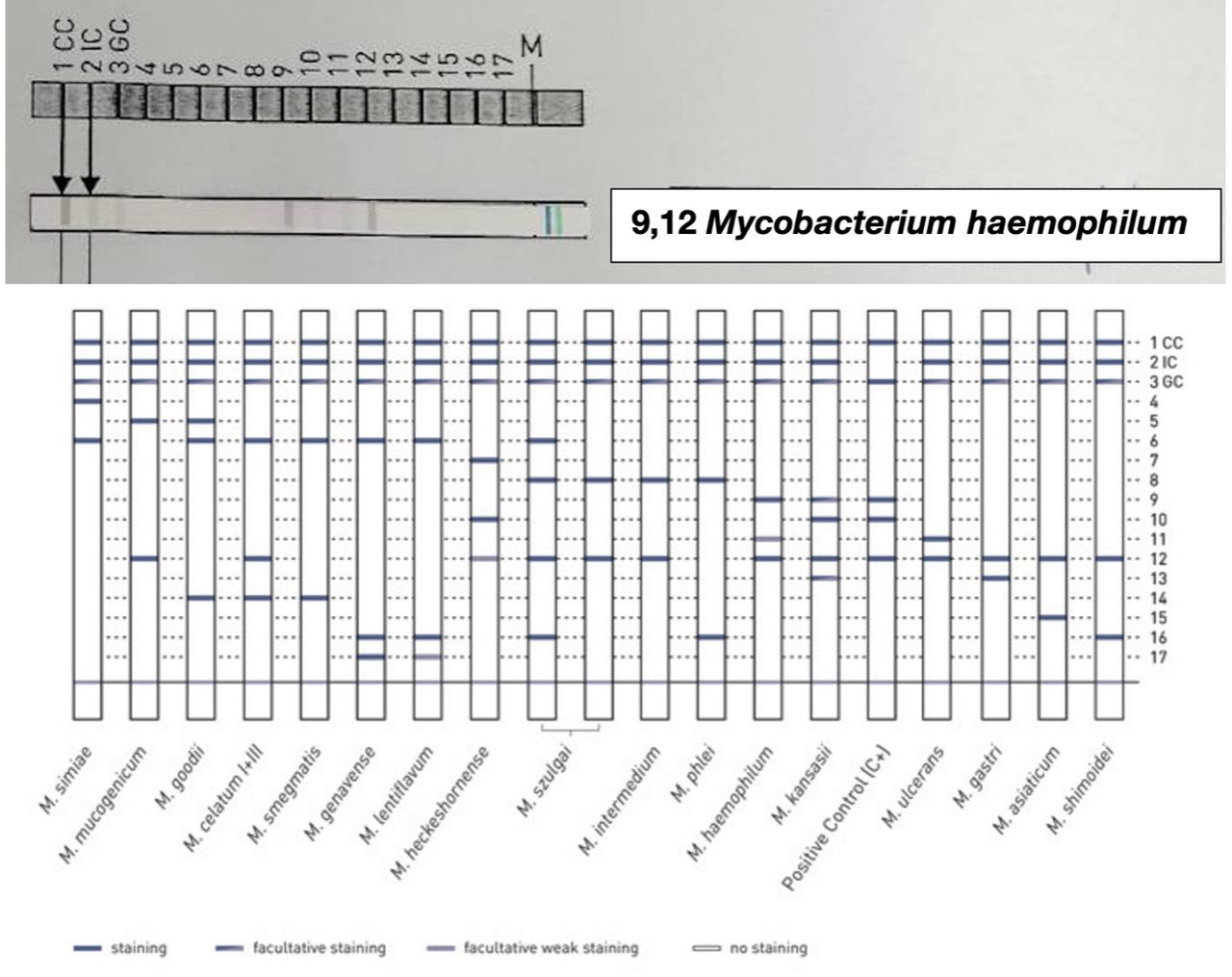
The analysis of the extracted corneal imprint revealed the presence of acid-fast bacilli, as shown by Kinyoun staining (figure 2A). Additionally, examination of the corneal section indicated an aggregation of lymphocytes and epithelioid histiocytes, visible with H&E staining (figure 2B). Kinyoun staining of the corneal section (figure 2C) also confirmed the ongoing presence of acid-fast bacilli within the stromal layer. The line probe assay (GenoType Mycobacterium AS 12, HAIN Life Science) verified the detection of M. haemophilum (figure 3).

Histopathology of the right cornea. Corneal imprint revealed acid-fast bacilli (A). Corneal section showed an aggregation of lymphocytes and epithelioid histiocytes (B) and confirmed acid-fast bacilli within the stromal layer (C).

Line probe assay yielded results compatible with the detection of Mycobacterium haemophilum.
Despite the absence of mycobacterial growth in the culture, the patient underwent a comprehensive phase treatment regimen. Treatment included systemic amikacin at 20 mg/kg three times per week, levofloxacin at 500 mg/day, rifampicin at 600 mg/day and azithromycin at 500 mg/day. This regimen was supplemented by topical antituberculous therapy, composed of topical 5% amikacin eyedrops administered four times per day and 0.5% moxifloxacin eyedrops administered four times per day, to enhance drug concentration within the corneal tissue.
Outcome and follow-up
On postoperative day 14, the patient exhibited improved visual acuity, including the ability to count fingers at a distance of 1 foot. Examination of the corneal graft revealed total haze and endothelial decompensation, with thinning observed from the 9 to 5 o’clock positions of the donor graft. No complications were noted during this period (figure 4A). Consequently, the patient was discharged from the hospital.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Follow-up eye examination (with the patient’s permission) postoperative day 14: total haze, endothelial decompensation and large epithelial defect in corneal graft (A). End of induction phase (8 weeks): total haze with peripheral thinning, intact central island with smaller epithelial defect and corneal neovascularisation (B). End of maintenance phase (10 months): total haze with peripheral thinning, neovascularisation, no epithelial defect and improved conjunctival injection (C).
Following 2 months of intensive phase treatment, the patient’s clinical condition exhibited marked stability, with the absence of recurrent keratitis, pus discharge and ocular discomfort. The patient maintained hand motion perception with a positive response to light projection. The examination, however, revealed complete haze of the corneal graft with 360 degree peripheral thinning, while the central island remained intact. Corneal neovascularisation was also observed. Although the epithelial defect on the cornea had improved and the progression of corneal thinning had ceased, indicating controlled infection, the graft exhibited total haze and was diagnosed as graft failure (figure 4B).
A decision then was made to transition to the maintenance phase of treatment due to the controlled infection. This phase involved administering levofloxacin at 500 mg/day, rifampicin at 600 mg/day and azithromycin at 500 mg/day for 12 months. Following the maintenance phase, the patient demonstrated hand motion vision with response to light projection in the superior and temporal directions. The graft displayed total haze with peripheral 360 degree thinning, neovascularisation and improved conjunctival injection (figure 4C).
The patient is awaiting a suitable donor for definitive corneal re-transplantation. Throughout the course of treatment, topical steroids were not administered at any point postoperatively.
Discussion
Our case showed M. haemophilum keratitis in a non-surgical cornea. Although this pathogen is an uncommon cause of keratitis, recurrent environmental exposure to contaminated water and the use of topical steroids appear to pose risks for infection.
To date, only four documented cases of M. haemophilum keratitis exist, with three reported in international medical databases and one from our presented case (table 1).5 9 10 The average patient age was 50 years, with 50% reporting no comorbidities. Only one of four cases involved a diabetic individual,9 indicating that the disease can affect healthy individuals without a compromised host.4 5 The nature of the disease is subacute or chronic, with a mean onset of 9.6 weeks. All available data reported topical steroid exposure before diagnosis, potentially elevating the risk of NTM infection.5 10 Uniquely, our case reports a history of recurrent environmental exposure to contaminated water suggesting a possible route and risk factor for infection acquisition.
Summary of the reported cases of Mycobacterium haemophilum keratitis
Regarding diagnostic methodology, only three cases are available. Acid-fast bacilli (AFB) have been observed on corneal histopathology5 rather than corneal scraping, indicative of the pathogen’s infiltration into the deeper layers of corneal tissue. Consistent with our case, the presence of AFB within the stromal layer of the cornea further substantiates the invasiveness of the pathogen. This occurrence aligns with the observation in the previous case report, highlighting the potential for negative microbiological findings in corneal scraping despite the actual presence of the pathogen.
PCR was able to detect all cases, with none diagnosed by conventional culture methods.5 10 PCR emerges as the most sensitive diagnostic modality for NTM keratitis and should be considered the gold standard. All M. haemophilum keratitis cases underwent treatment involving a combination of systemic and topical antimicrobials. In the three cases with successful treatment, the regimen was nearly identical, lasting at least 10 months.5 10 Systemic medications included macrolides, aminoglycosides, quinolones and rifampicin. Topical medications included quinolones, aminoglycosides, macrolides or rifampicin.5 10 Surgical management was essential for all cases to eradicate the disease,5 9 10 underscoring the invasiveness of the pathogen and the limited drug penetration in the cornea with both systemic and topical medication.
A key limitation of our case was the inability to produce mycobacterium growth, despite using mycobacterium culture in a low-temperature environment. Consequently, the standard antimicrobial sensitivity test could not be conducted. The diagnosis relied on PCR and a line probe assay. However, following empirical treatment with the standard M. haemophilum regimen, the patient exhibited a positive response to the treatment, indicating sensitivity of the disease to the prescribed drug.
In conclusion, M. haemophilum keratitis, though rare, can affect individuals with risk factors even in non-surgical or non-intervention cornea. Diagnosis poses challenges due to the invasiveness and difficulty in culturing the pathogen. Corneal surgery is preferred for obtaining microbiological evidence compared with corneal scraping. PCR appears to be the most sensitive method for diagnosis. A comprehensive treatment approach involving debridement surgery and a combination of systemic and topical anti-M. haemophilum medications administered over several months to a year appears to be the most effective treatment modality.
Patient’s perspective
Initially, I was worried that I might lose vision in my right eye. Despite undergoing multiple treatment regimens, my eye only seemed to worsen, experiencing increased irritation and redness. Eventually, I made the decision to undergo surgery to remove the infected cornea and replace it with a new one. It was only after the operation that I learnt about the specific bacteria causing the infection. There was a glimmer of hope for a cure. The doctors prescribed intravenous, oral and topical eyedrop antibiotics. Gradually, my right eye improved, with no irritation and reduced redness. Now, I can resume my daily activities, including housework and exercise. I eagerly await the next corneal transplantation, hoping for the restoration of brightness to my eye.
Learning points
Mycobacterium haemophilum is an uncommon cause of non-tuberculous mycobacterial keratitis.
Recurrent environmental exposure to contaminated water increases infection risk without prior corneal interventions.
Molecular techniques, especially PCR, are essential for diagnosis when prior treatment leads to negative conventional culture results.
Ethics statements
Patient consent for publication
Footnotes
Contributors The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content: PM, LU, UR and VN. The following authors gave final approval of the manuscript: PM, LU, UR and VN.
Funding This study was funded by Chulalongkorn University (DNS 64_002_30_001_2, DNS 66_007_30_001_3). The article processing fee was supported by Ratchadapiseksompotch Fund, Faculty of Medicine, Chulalongkorn University (RA-MF-53/64).
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.