Article Text

Abstract
Our patient is a woman who developed a subacute amnestic syndrome, followed by cognitive impairment, headache, temporal lobe epilepsy and hyponatraemia. An early-stage asymptomatic breast cancer was identified on positron emission tomography (PET) scan. After treatment with immunotherapy with high-dose corticosteroids, intravenous immunoglobulins, upfront rituximab and excision of the tumour, the patient gradually recovered. Partial retrograde and anterograde amnesia persisted during the initial weeks, followed by slow and steady improvement. Autoimmune encephalitis is a severe neurological disorder associated with antibodies against neuronal cell-surface or intracellular onconeural proteins. Anti-leucine-rich glioma inactivated 1 (LGI1) predominantly affects males in the seventh decade of life, and less than 10% of all cases are associated with cancer. Paraneoplastic cases have been associated with malignant thymoma, neuroendocrine tumours and mesothelioma and usually had Morvan syndrome, in which serum antibodies are more frequently directed against CASPR2 than against LGI1. We report the first well-documented case of anti-LGI1 limbic encephalitis in a woman with newly diagnosed breast cancer.
- Breast cancer
- Neurooncology
- Memory Disorders
- Clinical neurophysiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Autoimmune encephalitis (AE) encompasses a diverse array of inflammatory disorders affecting the central nervous system, with various causes and an intricate differential diagnosis.1 This severe clinical condition involves a misguided immune response, leading to the production of autoantibodies targeting self-antigens, with manifestations affecting the central nervous system.2
Autoimmune or paraneoplastic encephalitis (AE), while not common, is now more widely recognised thanks to the identification of specific antibodies (IgG) biomarkers (AE-Abs), which have significantly improved the diagnostic process.3 The exploration of antibodies targeting specific sites on the surface of neurons holds significant promise, as individuals possessing such antibodies may respond positively to immunological interventions.4 Unravelling the immune-neurological interplay is critical to advancing personalised and effective treatments for neurological disorders, including AE.
Cell surface antibodies and synaptic proteins, linked to the membrane via ADAM 22 or ADAM23, including anti-leucine-rich glioma inactivated 1 (LGI1)1 or contactin-associated protein-like 2 (CASPR2) antibodies, are usually associated with forms of limbic encephalitis (LE) that are generally non-paraneoplastic.5 LGI1 encephalitis is a treatable cause of AE. The clinical presentation includes cognitive impairment or rapidly progressive dementia, psychiatric disorders, faciobrachial dystonic seizures (FBDS), temporal focal seizures with or without impaired awareness and refractory hyponatraemia.6 The antibodies directed against LGI1 were described for the first time in 2010 by Irani et al7–9 The recognition of this entity has increased over the years, and the incidence appears to be on the rise. Two-thirds of individuals with LGI1 AE are males, typically between 50 and 70 years.10 11
Limbic encephalitis with LGI1-antibodies is the second most common cause of AE, following anti-N-methyl-D-aspartate receptor encephalitis.12 13 LGI1 encephalitis is noteworthy for its distinctiveness, most often occurring without any identifiable paraneoplastic cause.5 14 15 Nevertheless, some reports indicate that up to 11% of patients have a cancer-related origin, mainly presenting with thymoma or teratoma tumours.16
On the other hand, paraneoplastic neurological syndromes (PNSs) are defined as neurological disorders that can affect any part of the nervous system, often displaying stereotyped clinical manifestations. They occur in association with cancer and have an immune-mediated pathogenesis supported by the frequent presence of specific neuronal antibodies.15
PNS have a notably low prevalence in various neoplasms, such as breast or ovarian cancer, and other types of cancer, accounting for less than 1% of patients with a cancer diagnosis,17 and are most of the time related to onco-neuronal proteins Ma1, Ma2 and Ma3, which have been identified as antigens for paraneoplastic encephalitis.18
We describe an unusual case of LGI1 limbic encephalitis associated with breast cancer in a mid-40s previously healthy woman. This case report was prepared following the CARE guidelines.19
Case presentation
A previously healthy and asymptomatic white woman in her mid-40s sought neurological evaluation at the emergency room because of recent onset anterograde amnesia. She recounted testing positive for COVID-19 20 days before, with mild respiratory symptoms, fatigue and tiredness. One week later, her fatigue increased, accompanied by vivid and unfamiliar dreams, and the emergence of short-term memory loss.
She reported the onset of episodes resembling paroxysmal panic attacks 2 weeks before the consultation, occurring three times per week. These episodes, lasting 2–3 min, involved complete disorientation, crying and heightened anxiety without any external trigger, followed by an abrupt return to a normal state of mind. Additionally, she started having insomnia 2 weeks before her emergency room visit.
Her medical history included occasional asthma, severe pneumonia in her 20s, an appendectomy in 2020, and polycystic ovaries for which she received treatment with desogestrel, resulting in amenorrhoea.
Regarding her family history, the patient’s mother was successfully treated for breast malignancy in her 40s, with mastectomy, adjuvant chemotherapy and radiotherapy. Her maternal grandmother also had breast cancer around the age of 65 years. Because of her family history of breast cancer, the patient was regularly monitored by her gynaecologist, and she had normal mammography 16 months prior to her current hospitalisation.
The patient is married and holds a managerial position in the IT department at a bank. She has a history of smoking and has a sedentary lifestyle.
Clinical findings
The physical examination on the day of admission was normal except for obesity class II (BMI 35.1). The patient was disoriented in time and space, with anterograde amnesia, without any other focal neurological deficits. There were no meningeal signs, breast abnormalities or palpable adenopathy on physical examination. Furthermore, there were no reported paraneoplastic symptoms, such as unexplained weight loss or night sweats.
Investigations
Diagnostic assessment
Blood laboratory tests showed hyponatraemia at 133 mmol/L; other routine laboratory tests were unremarkable. Brain MRI conducted on the day of admission (figure 1) revealed hyperintensity and oedema in the left hippocampus on T2/FLAIR, with no abnormalities observed on diffusion-weighted imaging nor contrast enhancement. The cerebrospinal fluid (CSF) was clear, with two red blood cells and eight nucleated elements: 89% lymphocytes, 5% polymorphonuclear neutrophils and 6% monocytes. Protein and glucose levels, as well as protein isoelectric focusing and IgG index, were normal. The PCR meningitis/encephalitis multiplex panel for primary bacterial, viral and fungal pathogens (BioFire FilmArray) was negative.

MRI axial plane on top, down sagittal plane sequences T2/FLAIR FS: hyperintense signal and oedema in the left hippocampus.
Positive findings in serum included elevated anti-voltage-gated potassium channel antibodies (739 pmol/L) and anti-LGI1 antibodies (1/300). Other antibodies associated with encephalitis and anti-neuronal antibodies in serum and CSF, including anti-CASPR2 were negative. Anti-LGI1 antibodies in CSF were weakly positive (titre ½). Thyroid hormone levels, tumour markers (CEA, CA125, CA15.3, β-HCG) and C reactive protein were normal.
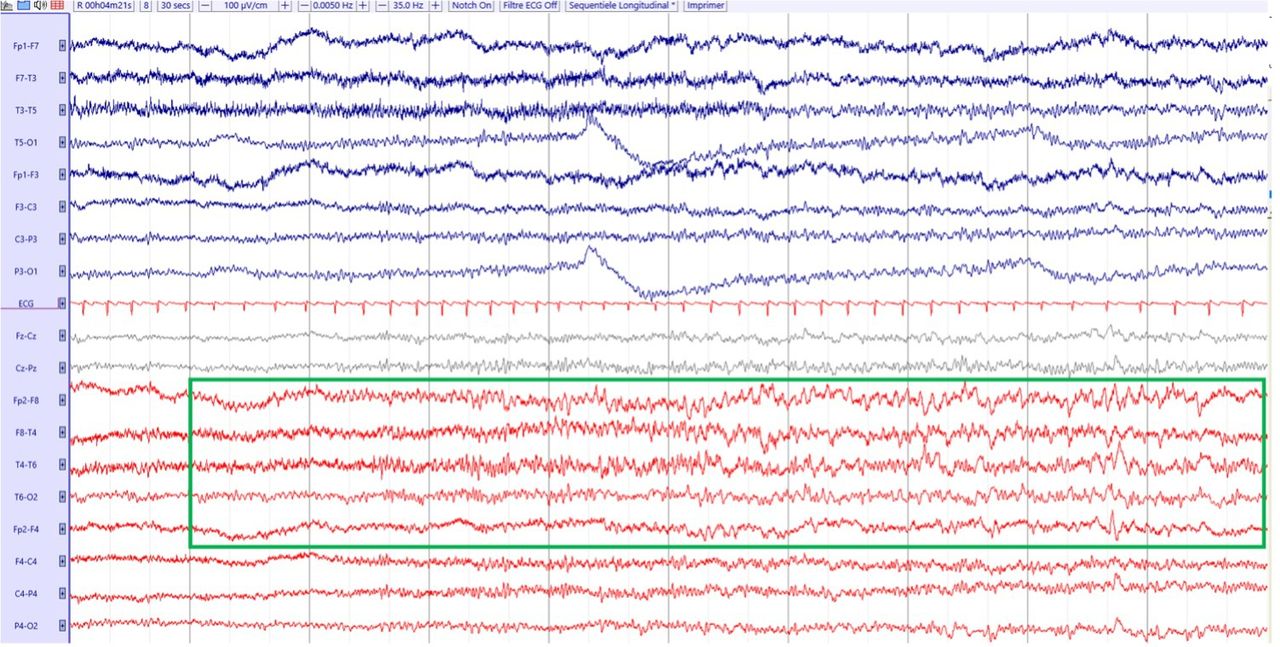
An EEG on the day of admission showed an irregular, slow background rhythm in the right temporal region. It also showed a focal seizure in the right temporal lobe without reported symptoms. Subsequent findings 3 days later showed right temporal interictal epileptiform spikes without documented seizures (figure 2).

EEG: focal seizure in the right temporal lobe.
The patient met three out of four criteria for the diagnosis of definite autoimmune limbic encephalitis:5 subacute onset of working memory deficits and seizures suggesting the involvement of the limbic system, unilateral brain abnormalities on T2-weighted FLAIR MRI highly restricted to the medial temporal lobe (bilateral required to meet the criteria), CSF pleocytosis, and EEG with epileptic and slow-wave activity involving the temporal lobe made at her admission. Positive anti-LGI1 antibodies in serum established the diagnosis of definite AE.
Treatment
The second day after her admission, we started treatment with intravenous immunoglobulins (Privigen), ceftriaxone, amoxicillin and acyclovir since it was not clear whether the encephalitis was infectious or inflammatory. In addition, she received lacosamide as an antiseizure medication. Once the multiplex and the different cultures came back negative, we switched to intravenous methylprednisolone 1 g per day for 5 days, followed by methylprednisolone tablets starting from day 6 at a dosage of 0,8 mg/kg/day for 1 month, with subsequent progressive taper.
Three days after admission and given concerns regarding severe amnesia in a professionally active young patient, standard infection screening was performed, including tests for hepatitis B, hepatitis C and tuberculosis, to ensure patient safety prior to the introduction of upfront rituximab 1000 mg intravenous infusions separated by 2 weeks, and pneumocystis preventive therapy with cotrimoxazole.
Outcome and follow-up
Clinically, the patient recovered gradually, with no recurrence of headaches or focal epileptic seizures since hospitalisation. Partial retrograde and anterograde amnesia persisted during the initial week, followed by a slow and steady improvement, and the patient returned to work with 80% of her previous time work 12 months after being discharged. Objective cognitive improvement was attested by a formal neuropsychological evaluation done at baseline and after 6 months of treatment. It included selective testing of verbal episodic memory by means of the Free and Cued Selective Reminding Test, and of visual episodic memory by means of recall of the Rey–Osterrieth complex figure.
A whole-body fluorodeoxyglucose-18 (FDG-18) positron emission tomography (PET) scan 2 weeks later (figure 3) revealed a moderately hypermetabolic lesion in the right breast. Histopathological analysis of a breast biopsy revealed a non-specific (ductal) infiltrative breast carcinoma, histoprognostic grade (SBRm/Nottingham) grade II (3-2-1), without ductal carcinoma in situ. The immunohistochemical study of hormone receptors and HER2/neu indicated the presence of oestrogen receptors (100%) and progesterone receptors (80%). The proliferation index was at 10%, and there was a low immunohistochemical overexpression of HER2 (score 1+).

{kind=link}
{kind=link}
{kind=link}
Positron emission tomography scan: moderately hypermetabolic lesion, approximately 15 mm from the junction of internal quadrants of the right breast (green arrow).
A lumpectomy of the tumour was performed 2 days later. The pathology report revealed an infiltrative breast carcinoma of mixed type, predominantly non-specific (80%) and a contingent of lobular type (20%), histoprognostic grade I (2-2-1) with a histological tumour size of 30 mm along the long axis. The lymphocytic stromal infiltrate was estimated at 10%, without endovascular carcinomatous emboli and no involvement of perineural sheaths. Ductal carcinoma in situ, intermediate grade, cribriform type, represented 10% of the total tumour surface. The immunohistochemical study of hormonal receptors and HER2/neu indicated the presence of oestrogen receptors (95%), progesterone receptors (80%) and a proliferation index estimated at 10%. There was no immunohistochemical overexpression of HER2 (score 0). Right axillary sentinel lymph nodes exhibited no metastasis (0/5). The pathological stage (UICC, eighth edition 2017) was determined as pT2 N0 (sn) G1 R.
Discussion
We describe the unusual case of a woman in her mid-40s with new diagnoses of LGI1 AE and concurrent breast cancer within a 3 week hospitalisation period. To the best of our knowledge, this is the first well-documented case of anti-LGI1 limbic encephalitis associated with early-stage breast cancer.
Strengths and limitations
The diagnosis of anti-LGI1 AE is well supported by a typical clinical picture as well as ancillary testing with MRI, EEG and positive anti-LGI1 antibodies. The availability of PET scan allowed for rapid identification and resection of the breast tumour with immunohistopathological analysis. Immunosuppressive treatment was started within 24 hours of admission.
PNS are characterised as disorders of the nervous system that can impact any area, typically displaying consistent clinical symptoms. These conditions are linked to cancer and have an immune-mediated mechanism supported by the frequent existence of particular neuronal antibodies. The three components of this description align with this specific case, indicating that it meets the diagnostic criteria for a PNS.15 However, applying the PNS care score proposed by Grau et al to categorise the likelihood of a PNS only leads to a score of 4, indicating a possible PNS (clinical level: 3 points, laboratory: 0, tumour level: not consistent with antibody, 1 point).
Limitations of case reports apply. Association is not causation. Given that breast cancer is common, that the patient has a family history of breast cancer, and the anti-LGI1 AE is rarely associated with cancer, it is possible that the two disorders occurred at the same time by chance. However, the close temporal relationship is striking and warrants further exploration of an association between anti-LGI1 AE and breast cancer.
An additional concern is that the patient had COVID-19 1 week before she noticed memory problems. There are several case reports of AE associated with COVID-19,20 including at least one possible post-infectious anti-LGI1 encephalitis complicating COVID-19.21 In the latter, the patient developed opsoclonus-myoclonus and encephalopathy associated with LGI-1 antibodies 6 days after the start of COVID-19 symptoms. Although there remains uncertainty about the significance of anti-LGI1 antibodies in the former case, there is a possibility that COVID-19 played a role in the case we describe, either by causing a post-infectious AE or as the final trigger in a paraneoplastic syndrome.
Finally, it is important to note that the detection of the LGI1 in the tumour sample was deemed unfeasible because it is a secreted protein rather than membrane-bound, and no specific antibody is currently commercially available for its in situ detection through immunohistochemistry.22 This lack of specificity may hinder efforts to analyse the distribution of LGI1 protein through immunohistochemistry, highlighting the need for further research in this area.
Relevant medical literature
The co-occurrence of paraneoplastic limbic encephalitis with breast cancer is uncommon. Among 137 reported cases of paraneoplastic limbic encephalitis, only four were associated with breast cancer.23 Individuals with breast cancer rarely have PNS, affecting an estimated 0.01% of the overall cancer patient population.24 PNS most commonly associated with breast cancer are subacute cerebellar degeneration, retinopathy, opsoclonus-myoclonus syndrome and Stiff-person syndrome.25
In the largest case series of breast cancer and LE published to this date, the autoantibodies detected were Purkinje cell cytoplasmic autoantibody type-1, amphiphysin-IgG, anti-neuronal nuclear autoantibody type-2, anti-acetylcholine receptor binding, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor, N-type anti-calcium channel, anti-glutamic acid decarboxylase-65 and unclassified antibodies.8
People with anti-LGI1 AE rarely have tumours. When they do, they are almost never breast tumours. In the largest published case series of anti-LGI1 AE, malignancy was reported in three out of 38 patients: a neuroendocrine pancreatic tumour, a thymoma with metastases and an abdominal mesothelioma.26
There are very few cases reported where breast cancer was diagnosed at the same time or even within the first year after the development of AE, and those cases were always related to non-LGI1-specific types of antibodies, including brain-testis-cancer antigens (Ma proteins anti-Ma2 or anti-Ta).18 Moreover, anti-LGI1 antibodies have never been described in relationship with breast cancer.
To the best of our knowledge, this may be the first documented case of breast cancer-associated anti-LGI1 AE. Additional features of interest include the close temporal relationship between the diagnosis of AE and breast cancer, as well as the age and gender of the patient. Anti-LGI1 AE predominantly affects men (60–65%) between the age of 55 and 80 years. The clinical manifestations align with expectations, featuring memory loss, hyponatraemia and temporal seizures as cardinal symptoms. Imaging revealed T2 hypersignal in the hippocampus, a characteristic observed in nearly 75% of patients with anti-LGI1 encephalitis.26
The patient responded well to prolonged corticosteroid therapy and early immunotherapy. Upfront rituximab was considered given the severe cognitive deficits and indirect evidence suggesting that IgG4-related diseases such as LGI1 encephalitis tend to have a good response to B cell-depleting therapies such as rituximab. The time from presentation to diagnosis and treatment was short, contrasting with reported cases where the typical time from symptom onset to the final diagnosis is considerably longer, taking in some cases more than 3 months.9
Conclusion
This case highlights the possible association between breast cancer and anti-LGI1 limbic encephalitis. In addition, it demonstrates that with increased awareness of AE and the availability of rapid antibody testing, it is possible to promptly make the diagnosis and initiate life-saving treatment.
Patient’s perspective
The information provided in this section was collected 4 months after the discharge of the patient.
The final week of my hospital stay is the only period I distinctly remember, leaving me uncertain about regaining memories from the last 3 years, which seem particularly obscured. Despite having theoretical knowledge, my recollections lack the vividness of lived experiences. This uncertainty extends to everyday memories, where I find myself doubting the authenticity of what I remember, including movies and books. However, I have noticed a gradual recovery in my cognitive abilities. An ongoing challenge is my difficulty in regulating emotions smoothly. The prospect of driving still feels daunting, though I am hopeful to partially resume work in a month.
Managing my medication has become a routine, with weekly organisation of my pill dispenser. Currently, I am undergoing hormonal treatment for breast cancer, striving to divert my thoughts from the memories I've lost to avoid distress. One of the most striking impacts of my condition is not remembering my daughter’s transition from childhood to adolescence. The realisation that a close friend passed away, without recalling our last encounter, deeply troubles me. Consequently, I rely heavily on my family to validate my memories, constantly questioning the accuracy of my recollections. Sleep disturbances and a consistent weight loss of approximately one kilogram per week further compound my challenges. Despite these difficulties, my hospitalisation was a period of relative well-being, although the prospect of discharge filled me with anxiety due to the unfamiliarity of returning to a home I couldn't remember. Paradoxically, moments of forgetfulness about my cancer diagnosis emerge as a fleeting respite. The experience of radiotherapy eludes me, yet the pervasive fatigue, exhaustion, and mood swings are undeniable.
My foremost concern lies in the potential permanent loss of memories from the past few years. This fear underscores the profound impact my illness has had on my personal identity and continuity of self. As I navigate this journey, the intersection of medical treatment and psychological adaptation remains a critical frontier, highlighting the intricate relationship between physical health and mental well-being.
Learning points
Auto-immune limbic encephalitis (AE LE) associated with anti-leucine-rich glioma inactivated 1 (LGI1) antibodies classically presents with an amnestic syndrome, faciobrachial seizures and hyponatraemia in older men. Less than 10% are associated with cancer, mostly lung, prostate and colon cancer.
This case of a woman in her 40s with LGI1 AE LE and breast cancer is a reminder for clinicians to remain open to the possibility of unusual presentations, and for researchers to explore this potential association.
The co-occurrence of paraneoplastic limbic encephalitis with breast cancer is uncommon. Among 137 reported cases of paraneoplastic limbic encephalitis, only four were associated with breast cancer.23 Individuals with breast cancer rarely have paraneoplastic neurological syndromes (PNSs), affecting an estimated 0.01% of the overall cancer patient population.24 PNS most commonly associated with breast cancer are subacute cerebellar degeneration, retinopathy, opsoclonus-myoclonus syndrome and Stiff-person syndrome.
Access to antibody testing and a high index of suspicion allowed for rapid initiation of steroids and rituximab, with good clinical outcomes.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All authors were directly involved in the patient’s care, drafting and revising the work, approved the final version to be published, and agree to be accountable for all aspects of the work. PK is the clinician in charge of the clinical care of the patient, who supervised the preparation of the manuscript, and is responsible for the overall integrity of the content of the manuscript. MFNU wrote the first draft of the manuscript, GVC was responsible for obtaining informed consent from the patient and family members, and acted as guarantor. Grammarly to correct english grammar errors, Zotero to cite the bibliography and Pubmed to search the bibliography.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.