Article Text

Statistics from Altmetric.com
Description
This case report highlights the challenges in diagnosing the rare endobronchial tuberculosis (EBTB) during the acute phase. The diagnostic dilemma escalated due to the fact that once airway stenosis has developed, it is irreversible and imposes significant morbidity and mortality.
We present a young Chinese woman in her twenties presented to the emergency department (ED) with noisy breathing and breathlessness. She was diagnosed with probable pulmonary tuberculosis (TB) with positive Mantoux and sputum examination for acid-fast bacilli and was started on anti-TB treatment a month prior. In ED, she was breathless, but the oxygen saturation was 95% under room air with normal vital parameters. Auscultations and chest radiograph were unremarkable. Upper airway assessment by the ear, nose and throat surgeon was normal. High-resolution (HR) CT thorax was performed in view of mild occasional stridor observed in the ward (figure 1). The HRCT revealed airway narrowing with bronchiectasis (figure 2) and mucous plugging (figure 3). Bronchoscopy performed showed caseating lesion in the right main bronchus (figure 4). Tracheal dilatation and mycotin injection were performed. Histopathological examination was suggestive of tuberculosis and confirmed by the culture.

Coronal view of reconstructive minimum intensity projection image showing tracheal stenosis narrowest at T4 level and narrowing in the right main bronchus.

Axial image in lung window revealed the right main bronchus narrowing with bronchiectatic changes in the anterior segment of the right upper lobe.

Axial image in mediastinal window depicted the right main bronchus endoluminal lesion with mucous plugging distally.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
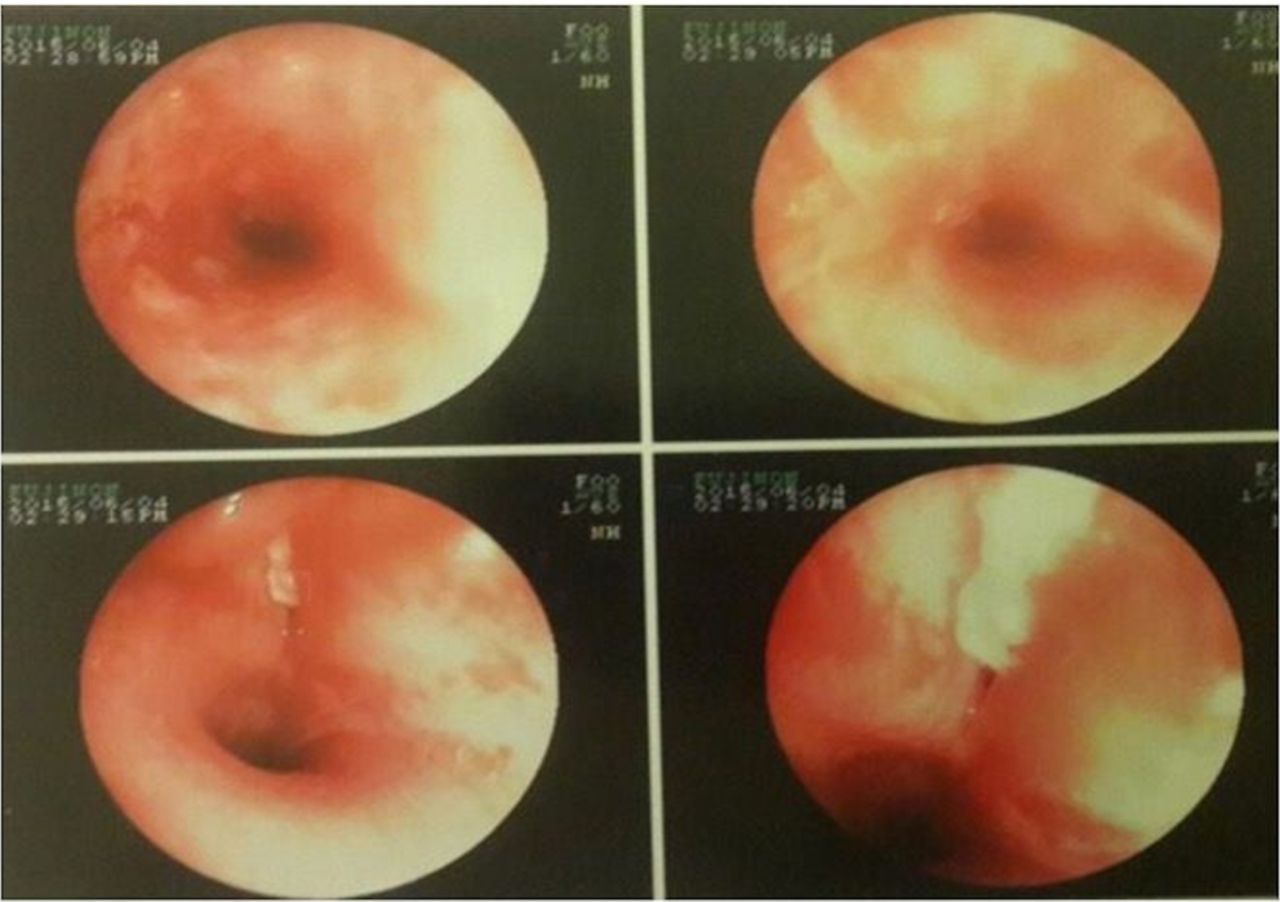
Bronchoscopy images with upper row showing trachea luminal narrowing and the bottom row showing caseating lesion at the right main bronchus.
The initial diagnosis of EBTB is a challenge. Furthermore, EBTB is known to have low sputum yield of 16%–53%.1 2 The definite diagnosis of EBTB is by HRCT and bronchoscopy, the latter having additional prognostication value.3 Chung classified EBTB into seven bronchoscopic subtypes: actively caseating, fibrostenotic, edematous-hyperaemic, tumorous, ulcerative, granular and non-specific bronchitic.1 The caseating type was seen in this case.
Learning points
Endobronchial tuberculosis (EBTB) is not often seen in the population nowadays after the advent of antituberculous therapy, and in most cases, it is associated with pulmonary tuberculosis. It has a special predilection for young female and geriatric population.1
Recognition of EBTB with subtle clinical presentation during acute phase is important because once significant stenosis has occurred, it is irreversible by antituberculous therapy and is life threatening.
The definite diagnosis of EBTB is by high-resolution computed tomography and bronchoscopy with histopathological examination, the latter having additional prognostication value.
Footnotes
Contributors Both authors contributed to the initial idea of the writing of the manuscript. The report and design of the manuscript were done by both authors. Reconstruction of the images and description done by HA.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.