Article Text

Abstract
This case report details a newborn in Ende, Indonesia, diagnosed with primary congenital lymphoedema, evidenced by bilateral lower limb swelling. This rare condition is characterised by developmental defects in the lymphatic system, leading to a fluid balance disruption. Diagnosis was primarily clinical, relying on thorough patient history and physical examination, given the limited resources for advanced diagnostic tools. The report emphasises the importance of supportive care, including meticulous skin care and manual lymph drainage, to improve life quality and minimise infection risks. It highlights the diagnostic and management challenges faced in low-resource settings and stresses the need for awareness and early intervention to manage such congenital conditions effectively.
- Congenital disorders
- Paediatrics
- Anatomic Variation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Lymphoedema is a condition characterised by the accumulation of protein-rich fluid due to disturbances in lymphatic circulation. The aetiology of lymphoedema is divided into two, primary and secondary.1 Primary lymphoedema is a genetic disease and syndrome, such as trisomy 13, 18, 21, Turner syndrome and other syndromes, that causes disruption of the lymphatic structure and function. Most primary lymphoedema occurs shortly after birth, but some also appear after the initial period of development.2 Meanwhile, secondary lymphoedema is caused by other causes or underlying diseases such as infection, kidney problems, tumours, postsurgery or radiotherapy.3
Approximately 90% of all cases of lymphoedema in children are primary cases. The prevalence of lymphoedema is reported to be 1.15/100 000 individuals aged less than 20 years. Symptoms of primary lymphoedema appear around infancy (49.2%), childhood (9.5%) and 41% adolescence. Primary lymphoedema often occurs in women with a ratio of 3.5:1. The prevalence of lymphoedema in teenagers is most often found in teenage girls compared with boys, with a ratio of 2:1, while in infancy, the prevalence of cases of lymphoedema most often occurs in baby boys with a ratio of 2:1. Epidemiological data is inadequate, including geographic areas or ethnic groups with higher incidence.4
Lymphoedema is usually characterised by swelling in one or more limbs. To diagnose primary lymphoedema, clinical assessment and an in-depth history can be carried out to exclude secondary risk factors. Other supporting examinations are still needed to ensure that there are no other secondary causes.
Ende is one of the districts in East Nusa Tenggara. Not many cases of lymphoedema in children have been reported in this area. In this case report, we present the case of primary congenital lymphoedema (PCL) and its approach to diagnosis and therapy in a limited resources area.
Case presentation
A baby girl was born by caesarean section transperitoneal delivery to a 30s mother at 40–41 weeks of gestation suffering from uterine myoma during pregnancy. She was born vigorously with a birth weight of 4100 g, a body length of 50 cm and a head circumference of 36 cm. There was no consanguinity between the mother and the father in the patient’s family history; the mother had no miscarriages or stillbirths, and they had two healthy children. The mother had a history of uterine myoma during pregnancy. There was no family inheritance disease related particularly to primary lymphoedema.
Investigations
On physical examination, we found severe bilateral swelling at the back of both the feet. There was bilateral swelling starting from the back of the foot and extending to the lower leg area below the knees. We noticed a positive Stemmer’s sign in the lower leg. The condition was no pitting oedema and cutaneous involvement (figure 1).

Swelling on the back of the foot extending to dorsum pedis bilateral. (A) Right foot, (B) whole body and (C) left foot. Author created.
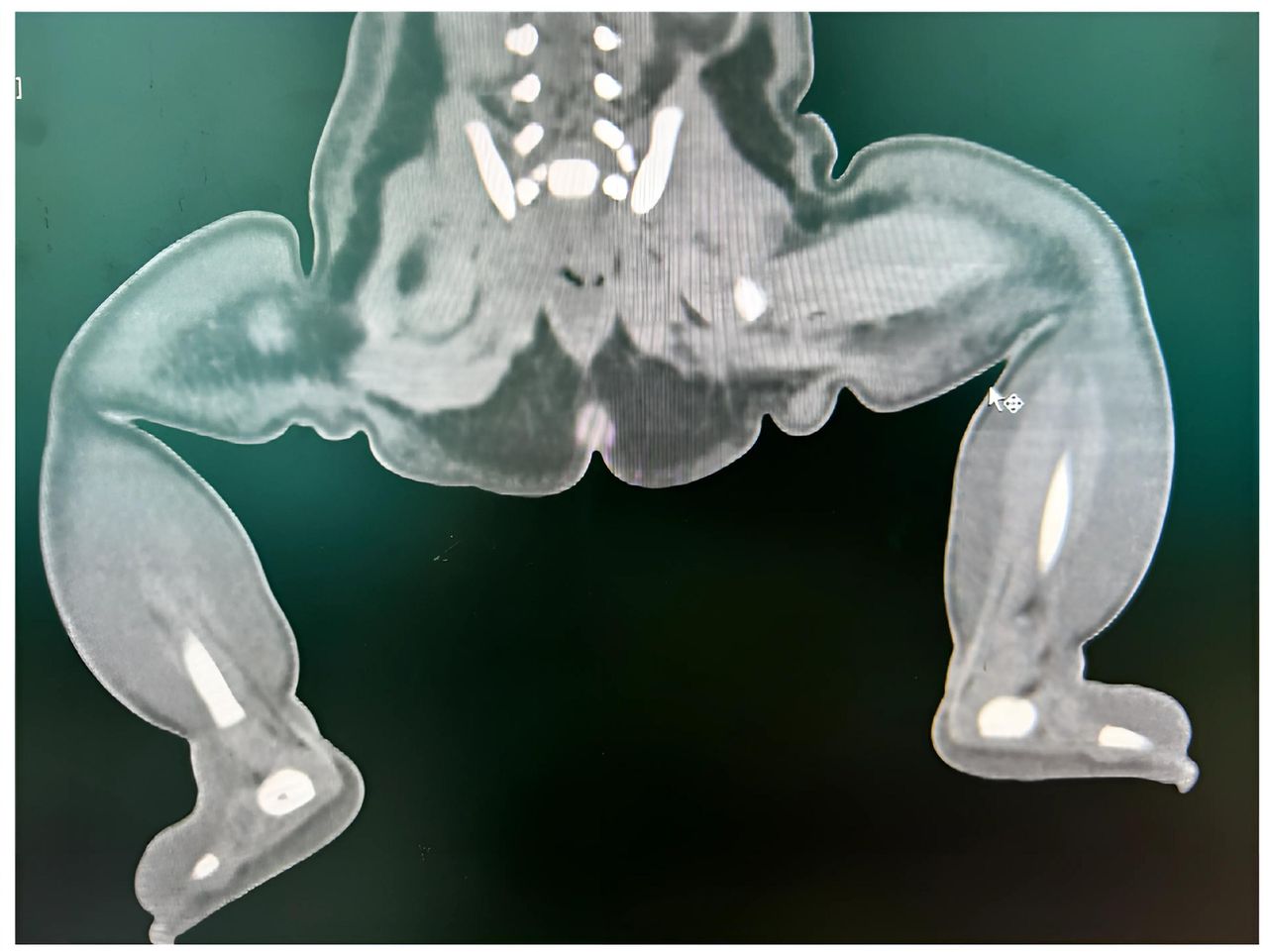
Laboratory findings on complete blood count, biochemical parameters and urinalysis to identify the cause of leg swelling revealed normal results. No pathological finding was found in the baby’s X-ray. Multislice CT (MSCT) revealed subcutaneous oedema that forms a honeycomb in the pelvic region, right and left femur, right and left cruris, and right and left foot, suggesting lymphoedema. No arterial and venous abnormalities were seen in the right and left inferior extremities. No bone or mass abnormalities were seen (figure 2).

Multislice CT (MSCT) bilateral pedis. The MSCT revealed subcutaneous oedema that forms a honeycomb in the pelvic region, right and left femur, right and left cruris, and right and left foot, suggesting lymphoedema. Author created.
Differential diagnosis
Lymphoedema can be either primary or secondary due to different acquired factors (infection, kidney failure), neoplasm, surgery and trauma. Based on history, there was no known major disorders or prenatal infection in the mother. There were no family members with a similar condition. Complete blood count, biochemical parameters, urinalysis, albumin, liver function test and renal function test were normal. There was no abnormality in the chest X-ray. MSCT revealed subcutaneous oedema suggesting lymphoedema with no arterial and venous abnormalities. We have not performed lymphoscintigraphy due to a lack of diagnostic modalities in a limited resources area. Primary lymphoedema is considered in this patient due to the absence of positive findings in all diagnostic examinations.
Treatment
Supportive therapy, such as keeping hydrated and applying moisturiser to protect the skin barrier in the affected area, was given.
Outcome and follow-up
In the monthly regular check-up, we have evaluated for complications, growth and development. There were no complications found in this patient. Assessment of growth and development was appropriate to her age. She started walking when she was 1 year, and her gait was normal. We continue to educate parents on how to care for their child’s feet to prevent trauma and secondary infection.
Discussion
Primary lymphoedema is caused by hypoplasia or aplasia of the lymphatic system, resulting in a decrease in intestinal fluid absorption and an increase in extremity volume. This process is usually followed by tissue changes such as thickening of the skin and increased fat deposits. Based on the age at which symptoms appear, primary lymphoedema is classified into three large groups, namely congenital lymphoedema (from birth to around 2 years), lymphoedema praecox (around 2–35 years) and late lymphoedema (>35 years).4 A summary of primary and secondary lymphoedema is listed in table 1 to distinguish between them.1 3–6
Primary versus secondary lymphoedema
The aetiology of primary lymphoedema is still unknown, but many articles state that genetics plays an important role in the occurrence of this case.3 4 In this case, the patient was born to a 30s mother, with a history of uterine myoma during pregnancy. According to a previous study, ageing causes a decrease in lymphatic function and lymphatic flow. This is caused by the disruption of muscle contraction, so that the pumping rate and pumping frequency decrease significantly, causing oedema.7 However, there has been no particular research discussing the relationship between pregnancy at old age and the incidence of primary lymphoedema in newborn babies. According to Pandit, the common complications experienced by babies born to mothers with uterine myoma are the threat of prematurity, intrauterine growth restriction, malpresentation and postpartum bleeding. This premature condition can cause a decrease in the function of the lymphatic blood vessels.8 9 However, in this case, the patient was born at term with a gestational age of 40–41 weeks. There are no articles that specifically discuss the history of pregnancy in mothers with myoma regarding the incidence of primary lymphoedema in newborn babies.
The clinical symptom that appears in patients with primary lymphoedema is swelling in one or more limbs. The skin was tighter on palpation. In some cases, it can be accompanied by pitting oedema, whereas others are not. On the back of the foot, it appears as a 'buffalo hump' caused by swelling, which is known to be a positive stemmer sign. This is in accordance with the clinical symptoms found in this patient.10 11 Cutaneous involvement may occur in primary lymphoedema, such as hyperpigmentation, hyperkeratosis, lymphorrhoea and papillomatous/verrucous lesions (figure 3). This condition is most common in children with an earlier onset.4 A perometer and a tape measure can be used to measure the volume of the limbs. Despite being the least accurate way to determine extremity volume, tape measurements can be particularly difficult for paediatrics because their limbs are still growing. Perometers are fast and accurate tools despite their high cost. A square frame with several perpendicular light beams is used in the technique. The cross-sectional area is continually estimated by moving the frame along the limb, and hence by volume.5 12 In this case, we found severe bilateral swelling on both dorsums of the feet. There was bilateral swelling starting from the dorsum of the feet and extending to the lower leg area below the knee with a positive Stemmer sign. The patient had no pitting oedema or cutaneous involvement. We did not perform perometer in our hospital because of the limited resources available in Ende.

Diagnostic algorithm for primary lymphoedema. Anamnesis, physical examination and supportive examinations, such as lymphoscintigraphy, are carried out to help confirm the patient’s diagnosis. Author created.
Given the numerous other conditions that can manifest as limb enlargement, diagnosis of lymphoedema can be challenging. Differential diagnoses for swelling in one or more limbs may include acquired factors (infection and kidney failure), neoplasm, surgery, trauma, lipoedema and other congenital disorders (vascular anomalies, lymphatic malformations, capillary or venous malformations, infantile haemangioma and kaposiform haemangioendothelioma) (table 2). Accurate diagnosis is important for proper management if a patient has lymphoedema.3 5 13 The diagnostic pearls of PCL are a patient with limb swelling with no underlying disease.4
Differential diagnosis of lower limbs swelling
Although the diagnosis of primary lymphoedema can be confirmed clinically and with a complete history, several examinations are still needed to rule out the cause of oedema in this case. Venous Doppler ultrasonography is necessary to exclude obstructions, such as thrombosis, and to identify avalvular venous insufficiency. A complete laboratory examination was performed to determine the presence of hypoalbuminaemia and proteinuria. Abdominal-pelvic CT was performed to exclude the possibility of secondary lymphoedema caused by the mass. Lymphoscintigraphy was the gold standard for confirming primary lymphoedema. In the event that no tumours or other disorders are discovered in the patient’s soft tissues or bones, lymphoedema is the diagnosis. To properly diagnose the patient, more tests can be carried out if the results do not indicate lymphoedema (figure 3).14 However, lymphoscintigraphy is not readily available for this purpose. CT is a widely available and easy to perform imaging tomography. MSCT is a more sophisticated CT. Because it uses several detectors, slices that are both thick and thin can be created. This implies that multiple slices can have data captured simultaneously and obtained in a shorter time.15 In this case, we performed a complete blood count, biochemical profile, urinalysis, baby gram X-ray and MSCT to rule out the possibility of lymphoedema secondary to a specific underlying disease. The laboratory examination results were normal. We did not perform venous Doppler ultrasound or lymphoscintigraphy in our hospital because of the limited resources available in Ende. Based on this examination, we concluded that the findings were suggestive of PCL after excluding the possibility of a secondary cause of lymphoedema in this patient.
The goal of lymphoedema management is to reduce and maintain volume, prevent complications, such as infection, and improve the patient’s quality of life.4 Lymphoedema can be divided into two different phases (figure 4). The first phase, also called complex decongestive therapy, aims to reduce the volume of lymphoedema and teach patients self-management to prevent infection. In this phase, actions that can be taken include wearing a low-stretch bandage, exercising while wearing a bandage, manual lymphatic drainage and care for the skin and nails with a moisturiser. The second phase, known as the maintenance phase, aims to maintain long-term stability of lymphoedema volume. In this phase, the action that can be taken is the use of additional compression to stabilise lymphoedema volume. No oral medications are available or recommended.3 In this case, the patient was a newborn baby. The initial treatment that can be done is to apply moisturiser three times per day in the intensive phase to keep the skin barrier moist and not dry, so that it does not become a source of infection, which then becomes cellulitis.16

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Management algorithm for primary lymphoedema. Lymphoedema can be divided into two different phases, namely, the first phase (complex decongestive therapy) and the second phase (maintenance phase). Author created.
The techniques for preventing complications include balanced and controlled daily physical activity, skin care and safeguarding against injuries, such as minimising pressure, needle sticking and temperature extremes.17 Primary lymphoedema requires constant monitoring by 6 months, especially lymphoedema with complications, which may require close monitoring. According to current studies, conservative therapy for PCL can reduce limb volume by 15%–30%. However, additional evidence is required for surgical interventions in this condition. Over the course of 5 years, 40%–60% of patients experienced cellulitis. Disease severity and response to treatment are influenced by genetic variables, including FLT4/VEGFR3 mutations. 20%–30% of patients still have persistent swelling after treatment, which emphasises the necessity for individualised care.18 Anamnesis, physical examination, management process evaluation, exercise interventions, and patient and/or family compliance must all be addressed during the routine check-up.5 In this case, the patient was evaluated for complications, growth and development monthly. There were no complications found in this patient.
Patient’s perspective
Having a child with congenital primary lymphoedema (CPL) has presented its fair share of challenges. Witnessing my child struggle with limb swelling, limited mobility, social judging, and discomfort was heartbreaking. Daily activities became hurdles, and their confidence seemed to dwindle.
However, seeing the improvement in their quality of life after starting treatment has been incredibly rewarding. Supportive treatments like applying emollient, using proper footwear, and exercising to perform mobilisation make movement easier and less frustrating. Their energy levels have risen, and they're participating more in playtime and activities they previously found difficult.
The emotional shift has been equally significant. My child seems happier and more confident. They're less self-conscious about their appearance and more willing to engage with others. While CPL remains a part of our lives, the improvement in their well-being makes it feel more manageable. It’s a constant reminder that even though there’s no cure, there are ways to manage the condition and create a fulfilling life for my child.
Learning points
Primary lymphoedema is associated with hypoplasia or aplasia in the lymphatic system, which causes an imbalance between the production and absorption of intestinal fluid in the lymphatic system.
Primary lymphoedema is mostly a clinical diagnosis after ruling out secondary causes of lymphoedema.
A detailed history and physical examination alone can accurately identify lymphoedema in approximately 90% of patients.
Diagnostic modalities remain a challenge in resource-limited areas such as Ende.
Supportive therapy for primary congenital lymphoedema will improve the quality of life and prevent secondary infections in patients.
Ethics statements
Patient consent for publication
Footnotes
X @Natashyangasu, @hayyurafina
Contributors The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigating results, drawing original diagrams and algorithms and critical revision for important intellectual content: DJY, NPN, HRS and BIRVC. The following authors gave the final approval of the manuscript: DJY, NPN, HRS and BIRVC. Guarantor: BIRVC.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.